ORIGINAL ARTICLE
Development and Evolution of a Diagnostic and Oral Pathology Service in a Southeast Brazilian State
Desenvolvimento e Evolução de um Serviço de Diagnóstico e de Patologia Bucal em um Estado do Sudeste Brasileiro
Desarrollo y Evolución de un Servicio de Diagnóstico y Patología Oral en un Estado del Sudeste Brasileño
doi: https://doi.org/10.32635/2176-9745.RBC.2022v68n2.2468
Laura Cruz-Mamani1; Marta Miyazawa2; Denismar Alves Nogueira3; Felipe Fornias Sperandio4; Alessandro Antônio Costa Pereira5; João Adolfo Costa Hanemann6
1-6Universidade Federal de Alfenas (Unifal). Faculdade de Odontologia. Alfenas (MG), Brazil.
4“University of British Columbia”, Faculty of Dentistry. Vancouver, BC, Canada.
1E-mail: arual_solyluna@hotmail.com. Orcid iD: https://orcid.org/0000-0002-6693-2893
2E-mail: mkmiyazawa@yahoo.com.br. Orcid iD: https://orcid.org/0000-0001-8529-2441
3E-mail: denisnog@gmail.com. Orcid iD: https://orcid.org/0000-0003-2285-8764
4E-mail: ffsperandio@gmail.com. Orcid iD: https://orcid.org/0000-0003-3134-7659
5E-mail: aac.pereira@uol.com.br. Orcid iD: https://orcid.org/0000-0002-2763-8405
6E-mail: jachanemann@uol.com.br. Orcid iD: https://orcid.org/0000-0002-3865-905X
Corresponding author: João Adolfo Costa Hanemann. Unifal. Faculdade de Odontologia. Rua Gabriel Monteiro da Silva, 700 ‒ Centro. Alfenas (MG), Brazil. CEP 37130-001. E-mail: jachanemann@uol.com.br
ABSTRACT
Introduction: Oral squamous cell carcinoma (OSCC) is one of the most frequent cancers whose main causes are preventable because oral cavity is easily accessible for examination. OSCC involves many steps from the diagnosis until treatment which can result in late diagnosis and worst prognosis. Objective: Development and evolution of a Stomatology and Oral Pathology Service at the Federal University of Alfenas addressing early diagnosis and management of oral lesions. Method: Retrospective study developed with the files from 1998 to 2019. Data from all the cases diagnosed as oral malignancies were collected and the demographical, clinical, and microscope diagnosis were included. Results: 270 (84.64%) OSCC were found among 8,952 histopathological diagnoses. The patients age ranged from 24 to 94 years (mean 59.7±13.1 years), and more frequent in the sixth (32.3%) and seventh (26%) decades of life. Men were 2.5 times more affected than women. Most of patients were Caucasian (74.8%), and users of tobacco and alcohol. Over the years, there was an increase in the number of cases diagnosed and expansion of the area covered by the Service. Conclusion: The Dental Clinic (Stomatology) and Oral Pathology Laboratory has been playing an important role for the establishment and improvement of the healthcare system to the local population, mainly in rural areas.
Key words: mouth neoplasms/diagnosis; carcinoma, squamous cell; early diagnosis; health services.
RESUMO
Introdução: O carcinoma de células escamosas (CEC) de boca está entre os cânceres mais frequentes. Suas principais causas são evitáveis, pois a cavidade oral é uma área de fácil acesso para exame. No entanto, desde o estabelecimento do diagnóstico até o tratamento final dos pacientes, o CEC envolve muitas etapas e pode resultar em diagnóstico tardio e, portanto, em pior prognóstico para os pacientes. Objetivo: Apresentar o desenvolvimento e a evolução de um Serviço de Estomatologia e Patologia Oral da Universidade Federal de Alfenas, que tem como foco o diagnóstico precoce e o tratamento de lesões bucais. Método: Estudo retrospectivo com os prontuários de 1998 a 2019. Foram coletados dados de todos os casos diagnosticados como malignidades orais e incluídos os diagnósticos demográficos, clínicos e microscópicos. Resultados: Entre 8.952 diagnósticos histopatológicos realizados, 270 (84,64%) eram CCE. A idade dos pacientes variou de 24 a 94 anos (média 59,7±13,1 anos), sendo mais frequente na sexta (32,3%) e sétima (26%) décadas de vida. Os homens foram 2,5 vezes mais afetados do que as mulheres. A maioria dos pacientes era branca (74,8%) e o uso de tabaco e álcool, frequente. Ao longo dos anos, houve um aumento no número de casos diagnosticados, bem como uma ampliação da área de cobertura do Serviço. Conclusão: O Serviço de Estomatologia e Patologia Oral tem desempenhado um papel importante na implantação e melhoria do sistema de saúde da população local, principalmente nas Regiões interioranas e em áreas rurais.
Palavras-chave: neoplasias bucais/diagnóstico; carcinoma de células escamosas; diagnóstico precoce; serviços de saúde.
RESUMEN
Introducción: El carcinoma de células escamosas (CCE) de boca se encuentra entre los cánceres más frecuentes. Sus principales causas se pueden prevenir ya que la cavidad bucal es un área de fácil acceso para su examen. Sin embargo, desde el establecimiento del diagnóstico hasta el tratamiento final de los pacientes, la CEC implica muchos pasos y puede resultar en un diagnóstico tardío y, por lo tanto, un peor pronóstico para los pacientes. Objetivo: Presentar el desarrollo y evolución de un Servicio de Estomatología y Patología Bucal de la Universidad Federal de Alfenas que se enfoca en el diagnóstico y tratamiento precoz de las lesiones bucales. Método: Estudio retrospectivo con historias clínicas de 1998 a 2019. Se recolectaron datos de todos los casos diagnosticados como neoplasias bucales, incluyendo diagnósticos demográficos, clínicos y microscópicos. Resultados: De los 8952 diagnósticos histopatológicos realizados, 270 (84,64%) fueron CCE. La edad de los pacientes osciló entre 24 y 94 años (media 59,7±13,1 años), siendo más frecuente en la sexta (32,3%) y séptima (26%) décadas de la vida. Los hombres se vieron 2,5 veces más afectados que las mujeres. La mayoría de los pacientes eran de raza blanca (74,8%) y el consumo de tabaco y alcohol era frecuente. A lo largo de los años, ha habido un aumento en el número de casos diagnosticados, así como una expansión del área de cobertura del Servicio. Conclusión: El Servicio de Estomatología y Patología Bucal ha jugado un papel importante en la implementación y mejora del sistema de salud para la población local, especialmente en las Regiones del interior y áreas rurales.
Palabras clave: neoplasias de la boca/diagnóstico; carcinoma de células escamosas; diagnóstico precoz; servicios de salud.
INTRODUCTION
In Brazil, oral squamous cell carcinoma (OSCC) is predominant in males between 50 and 60 years old, mainly in the lateral and ventral tongue and floor of the mouth1-7. Tobacco and alcohol use and low life standards are the main risk factors2,4,6-9. The country’s high mortality rates are explained by the diagnosis usually at more advanced stages which hampers appropriate treatment, making cure more unlikely1,2,4,6-10. The low level of education has also been associated with increased oral cancer incidence, particularly in advanced cases5,7,9.
The state of Minas Gerais (MG) belongs to the Brazilian Southeast region, it has the highest incidence of oral cancer in the country8,10. According to the estimates of the National Cancer Institute José Alencar Gomes da Silva (INCA)11 for 2020, 1,620 new cases of oral malignant neoplasm are anticipated for the state, the incidence for males is 9.21-11.17 cases per 100,000 inhabitants, and 2.01-2.69 for females.
The Bayesian model-based evaluation of death rate in MG to find more accurate data on oral and oropharynx cancer mortality identified accumulation of cases in the North, Central, and South regions of the state. The crude rate showed that Alfenas, a southern city of MG, presented 0.01-10.12 deaths per 100,000 inhabitants, and the Spatial Empirical Bayesian rate showed 5.57-36.85 deaths per 100,000 inhabitants12.
Oral cancer studies developed in Belo Horizonte, the state’s capital, concluded that typically the population at risk for oral cancer is found in the poorest social classes. There was higher prevalence in males (4 to 5:1) with mean age around 60 years, tobacco and alcohol users, mostly at the tongue and floor of the mouth at advanced stages1,13 with prolonged time of evolution1.
More recently, a social-spatial analysis of a public hospital at Belo Horizonte, concluded that individual economic status and geographical area of residence are important factors related to the disparities in the prevalence of oral cancer13. The population was interviewed about what level of knowledge they had about oral cancer, revealing that dentists are important sources of information, providing guidance on prevention and drawing attention to the etiology of the disease14.
Along the years, the Brazilian public health system has been improving and has become more accessible in less developed areas far from the capital. Therefore, the aim of this study is to present the evolution of the Dental Clinic (Stomatology) and Oral Pathology Service along its 22 years of existence at the Federal University of Alfenas, MG, Brazil and its significant contribution for the local community, mostly for patients with oral cancer.
METHOD
A retrospective study developed with the files of the Oral Pathology Laboratory of the Federal University of Alfenas (Unifal), from 1998 to 2019. Data from all the cases diagnosed as oral malignancies were collected and included: demographical (age, gender, race, tobacco and alcohol use, city of origin), clinical (anatomic site and aspect of the lesion), and microscopic diagnosis. In addition, the cases were divided in two periods (1998-2006 and 2007-2019) to evaluate the development of the Service and compared with a previous study developed by the group15.
Hematoxylin-eosin-stained slides were used to review all the cases. Diagnosis included oral squamous cell carcinoma, verrucous carcinoma, malignant salivary gland neoplasia and others. An optical microscope (AxioLab ‒ Carl Zeiss, Göttingen, Germany) with the objective N-Achroplan 40X/0,65, with final 400X was utilized for morphological analyzes. Two blind experienced reviewers developed two independent analyses. OSCC cases included in this study were classified according to El-Naggar et al.16 as Grade I or well differentiated, Grade II or moderately differentiated and Grade III or poorly differentiated.
All data collected were analyzed statistically with STATA version 16.0 (StataCorp LP, College Station, Texas)17. Distribution of frequencies was used to describe categorical variables (number of cases and relative percentage), and measures of central tendency (mean and median) and variability (minimum, maximum and standard deviation) for numerical variables. To compare the groups with two categories ("Year") for age, Student's T-Test was applied; for categorical variables, the chi-square test was used for comparison between the groups, and when the expected frequency was <5, Fisher Exact Test was used. The verification of normality of the data was developed with Shapiro-Wilk test. Significance level was set at 5% (p≤0.05).
The Institutional Review Board of Unifal (CAAE: 24091519.6.0000.5142) approved the study.
RESULTS
Among 8,952 histopathological diagnoses from January/1998 to December/2019 at the Oral Pathology Laboratory – Federal University of Alfenas, 319 cases (3.56%) were of oral malignant neoplasia. Among these cases, 270 (84.64%) were oral squamous cell carcinoma (OSCC), 21 (6.58%) were malignant salivary gland neoplasia, 19 (5.96%) verrucous carcinoma, 6 (1.88%) sarcomas, 2 (0.63%) lymphomas, and one (0.31%) melanoma. The other 8,633 cases comprise inflammatory and infectious diseases and non-malignant neoplasms.
Considering the increasing number of patients with oral cancer diagnosed at the Federal University of Alfenas, the patient profile was also evaluated for better understanding of the role this Public Health Service plays in the community. The distribution of OSCC cases according to the year of diagnosis showed that 2017 had the highest number (27 cases), followed by 2013 and 2019 (25 cases each). The analysis of the frequency of cases during the interval 1998-2006, when the first study of the Service was developed15, versus 2007-2019, showed high increase in the mean number of cases of OSCC per year from 4.7 cases/year to 17.5 cases/year, respectively (Table 1).
The age of the patients ranged from 24 to 94 years (mean 59.7±13.1 years) (Table 1), and more frequent on the sixth (32.3%) and seventh (26%) decades of life. Men were 2.5 times more affected than women. Most patients were Caucasian (74.8%), and users of tobacco and alcohol. The predominant locations of the tumor were tongue (32.2%), floor of the mouth (24.4%) and gingiva/alveolar ridge (19.4%); clinically, most of the lesions presented as ulcers (Table 1).
The biopsies forwarded by the dentists of the community off-University failed to present data about the patients' habits such as tobacco and alcohol use, and location of the lesion, hampering the analysis of these variables (Table 1).
Along the years, different descriptive terms for OSCC could be identified (Table 1), therefore a complete review of all the cases and reclassifications according to El-Naggar et al.16 was developed to eliminate bias of histopathological diagnosis. It revealed that the sample consisted of 116 cases (43.0%) of Grade I or well differentiated SCC, 145 (53.7%) of Grade II or moderately differentiated SCC, and only 9 (3.3%) of Grade III or poorly differentiated SCC (Table 2).
In order to evaluate the evolution of the patient profile diagnosed at the Oral Pathology Laboratory of Unifal, they were categorized as before and after 2006 (Tables 3 and 4). The demographical profile of the patients did not change. However, there was a tendency towards the change of the frequency of tumor anatomic location from gingiva/alveolar ridge to tongue and floor of the mouth. In addition, it seems that the off-University dentists have improved their clinical description of the lesions sampled for histopathologic analysis; for example, the general descriptive term "ulcer/ulceration" have been more specifically termed "infiltrative ulcer" (Table 3). The histopathological diagnoses changed significantly because earlier they did not specify the degree of OSCC differentiation (Table 3).
Over the years, the number of cases diagnosed increased as well as the Service’ coverage area, in terms of the origin of the patients. To better understand this scenario, the patients were classified according to the State Health Regional Superintendence (SRS).
Until 2006 the patients were predominantly from SRS Varginha (52.9%) and SRS Alfenas (29.4%), and none of the cases from other Brazilian States. From 2007, there is a clear inversion of this profile by means of SRS Alfenas having 47.8% and SRS Varginha 24.4% of the cases, as well as an expansion of the covered area with patients residing in other SRS of the State (SRS Passos, Pouso Alegre, Varginha, Divinópolis, Itabira, Manhuaçu, Sete Lagoas, and Ubá) and São Paulo State (4 cases) (Table 4). The distribution of the cases during these two periods can be observed in Figure 1, showing the increasing number of regional cases and a clear expansion of the cases in the State.
When cases only from MG are analyzed comparing the two periods, it can be observed that in 1998-2006, 70.6% of the cases were not from SRS Alfenas despite the location of the Service, and today this SRS represents 48.8% of the cases. This significant change (p=0.036) shows the importance of the Service for the local population (Table 4).
|
Table 1. Distribution of the patients according to demographical and clinical variables (N=270) |
||
|
Variable |
Category |
Frequency (%)/Measures |
|
1998-2006 |
42 (15.6) |
|
|
2007-2019 |
228 (84.4) |
|
|
Age (years) |
N |
254 |
|
Variation |
24-94 |
|
|
Median |
59 |
|
|
Mean (Standard deviation) |
59.7 (13.1) |
|
|
Gender |
Male |
193 (71.5) |
|
Female |
77 (28.5) |
|
|
Race |
Caucasian |
166 (74.8) |
|
Non-Caucasian |
29 (13.1) |
|
|
Black |
27 (12.2) |
|
|
Tobacco use (N=63) |
No |
3 (4.8) |
|
Yes |
60 (95.2) |
|
|
Alcohol use (N=45) |
No |
4 (8.9) |
|
Yes |
41 (91.1) |
|
|
Location (N=258) |
Lower lip |
31 (12.0) |
|
Tongue |
83 (32.2) |
|
|
Floor of the mouth |
63 (24.4) |
|
|
Gingiva/Alveolar ridge |
50 (19.4) |
|
|
Palate |
26 (10.1) |
|
|
Buccal mucosa |
5 (1.9) |
|
|
Clinical aspect of the lesion (N=237) |
Superficial ulcer |
13 (5.5) |
|
Infiltrative ulcer |
78 (32.9) |
|
|
Vegetative ulcer |
15 (6.3) |
|
|
Nodule |
14 (5.9) |
|
|
Leukoplakia |
24 (10.1) |
|
|
Erythroplakia |
17 (7.2) |
|
|
Ulcer/Ulceration |
76 (32.1) |
|
|
Histopathological diagnosis (N=270) |
SCC in situ/invasive |
30 (11.1) |
|
SCC well differentiated |
33 (12.2) |
|
|
SCC moderately differentiated |
93 (34.4) |
|
|
SCC |
114 (42.2) |
|
|
Captions: SCC = Squamous cell carcinoma. |
||
|
Table 2. Distribution of the patients according to clinical and pathological variables (N=270) |
||
|
Variable |
Category |
Frequency (%) |
|
SCC Grade I |
116 (43.0) |
|
|
SCC Grade II |
145 (53.7) |
|
|
SCC Grade III |
9 (3.3) |
|
|
SRS (N=239) |
Alfenas |
108 (45.2) |
|
Passos |
5 (2.1) |
|
|
Pouso Alegre |
40 (16.7) |
|
|
Varginha |
68 (28.4) |
|
|
Other SRS* |
14 (5.9) |
|
|
Other State |
4 (1.7) |
|
|
Captions: SCC = Squamous cell carcinoma; SRS = Health regional superintendence. (*) Divinópolis, Itabira, Manhuaçu, Sete Lagoas, and Ubá. |
||
Table 3. Distribution of demographical and clinical variables according to the year (N=270)
|
Variable |
Category/ Measures |
YEAR |
p-value# |
|
|
1998-2006 2007-2019 |
||||
|
Measure/Frequency (%) |
||||
|
N |
40 |
214 |
0.832 |
|
|
Variation |
31-85 |
24-94 |
||
|
Median |
56.5 |
59.5 |
||
|
Mean (Standard deviation) |
59.3 (14.2) |
59.8 (12.9) |
||
|
Gender |
Male |
27 (64.3) |
166 (72.8) |
0.261* |
|
Female |
15 (35.7) |
62 (27.2) |
||
|
Race (N=222) |
Caucasian |
21 (61.8) |
145 (77.1) |
0.106* |
|
Non-Caucasian |
8 (23.5) |
21 (11.2) |
||
|
Black |
5 (14.7) |
22 (11.7) |
||
|
Tobacco use (N=63) |
No |
0 (0.0) |
3 (5.7) |
>0.05** |
|
Yes |
10 (100.0) |
50 (94.3) |
||
|
Alcohol use (N=45) |
No |
0 (0.0) |
4 (10.3) |
>0.05** |
|
Yes |
6 (100.0) |
35 (89.7) |
||
|
Location (N=258) |
Lower lip |
5 (12.8) |
26 (11.9) |
NA |
|
Tongue |
8 (20.5) |
75 (34.2) |
||
|
Floor of the mouth |
5 (12.8) |
58 (26.5) |
||
|
Gingiva/Alveolar ridge |
12 (30.8) |
38 (17.4) |
||
|
Palate |
6 (15.4) |
20 (9.1) |
||
|
Buccal mucosa |
3 (7.7) |
2 (0.9) |
||
|
Clinical aspect of the lesion (N=237) |
Superficial ulcer |
1 (2.9) |
12 (5.9) |
NA |
|
Infiltrative ulcer |
6 (17.7) |
72 (35.5) |
||
|
Vegetative ulcer |
3 (8.8) |
12 (5.9) |
||
|
Nodule |
0 (0.0) |
14 (6.9) |
||
|
Leukoplakia |
3 (8.8) |
21 (10.3) |
||
|
Erythroplakia |
3 (8.8) |
14 (6.9) |
||
|
Ulcer/Ulceration |
18 (52.9) |
58 (28.6) |
||
|
Histopathological diagnosis (N=270) |
SCC in situ/invasive |
4 (9.5) |
26 (11.4) |
<0.001* |
|
SCC well differentiated |
19 (45.2) |
14 (6.1) |
||
|
SCC moderately differentiated |
15 (35.7) |
78 (34.2) |
||
|
SCC |
4 (9.5) |
110 (48.3) |
||
|
Captions: SCC = Squamous cell carcinoma; NA = statistically not available. (#) p-value by Student's T test. (*) p-value by chi-square frequency test. (**) p-value by Fisher's exact test. |
||||
Table 4. Distribution of clinical and pathological variables according to the Year (N=270)
|
Variable |
Category |
YEAR |
p-value# |
||
|
1998-2006 |
2007-2019 |
||||
|
Measure/Frequency (%) |
|||||
|
SCC Grade I |
21 (50.0) |
95 (41.7) |
NA |
||
|
SCC Grade II |
19 (45.2) |
126(55.3) |
|||
|
SCC Grade III |
2 (4.8) |
7 (3.1) |
|||
|
SRS (N=239) |
Alfenas |
10 (29.4) |
98 (47.8) |
NA |
|
|
Passos |
0 (0.0) |
5 (2.4) |
|||
|
Pouso Alegre |
3 (8.8) |
37 (18.0) |
|||
|
Varginha |
18 (52.9) |
50 (24.4) |
|||
|
Other SRS* |
3 (8.8) |
11 (5.4) |
|||
|
Other State |
0 (0.0) |
4 (2.0) |
|||
|
SRS-MG |
Alfenas |
10 (29.4) |
98 (48.8) |
0.036 |
|
|
Other SRS** |
24 (70.6) |
103 (51.2) |
|||
|
Captions: NA = statistically not available; SRS = Health regional superintendence. (#) p-value by chi-square frequency test. (*) Divinópolis, Itabira, Manhuaçu, Sete Lagoas, and Ubá. (**) Passos, Pouso Alegre, Varginha, Divinópolis, Itabira, Manhuaçu, Sete Lagoas, and Ubá. |
|||||
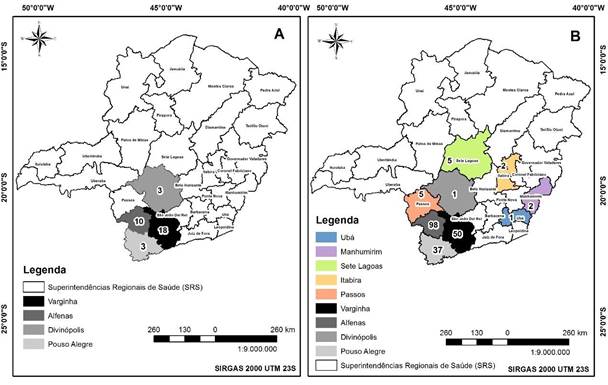
Figure 1. Representation of the Health Regional Superintendence (SRS) of Minas Gerais State18 and the distribution of the cases of OSCC from the Oral Pathology Laboratory ‒ Unifal during the periods A) 1998-2006 and B) 2007-2019
DISCUSSION
The National Health System (SUS) was created in 1990 and it is a public health system with universal access for the population. It is based on decentralization, creating health regions with integrated health planning by means of regional management boards under the supervision of health state secretariats in partnership with municipal authorities19. Thereby, MG is divided into 18 Health Regional Superintendence (SRS) and 10 Health Regional Management (GRS)18. The present Service belongs to SRS Alfenas.
Primary health care is the main access to SUS, providing primary (control of risk factors) and secondary prevention (early detection) for oral and oropharyngeal cancer. The increasing number of dentists in primary care resulted in early detection of oral cancer, easily screened at clinical examination where suspicious lesions are able to be identified visually20. However, the access to specialists remains a major bottleneck resulting in unmet demands, queues, long waiting times, and diagnoses2,19 delays.
Through this system, the final diagnosis of oral and oropharyngeal cancer is to be performed on the Specialized Dental Care (SDC) centers. When the primary care dentist detects a potentially malignant oral lesion, the Oral Health Team is expected to refer the patient to a SDC, where a biopsy will be run and later to a hospital for cancer treatment, if needed20.
In this scenario, the Dental Clinic (Stomatology) at the Dental School and the Oral Pathology Laboratory of the Unifal plays an important role on oral cancer diagnosis for the local community whose main economic activity is agriculture. In addition, this region is 350km far from the State’s capital. Once the patients receive a cancer diagnosis at the Service, they can proceed to the nearest SUS healthcare system available for subsequent treatment.
The first study to evaluate the present Service included the OSCC cases reported in the period of 1998-200615; there were no significant differences in demographical, clinical, and histopathological data between the first period and the current period of 2007-2019 (Tables 3 and 4), and the patient profile is compatible with other previous Brazilian studies (Table 1) – male, around 60 years of age, tobacco and/or alcohol user, advanced tumors in the tongue or floor of the mouth1-7. Nevertheless, the data analysis was flawed because many off-University dentists forwarded the biopsies without data of the patient’s use of tobacco and alcohol and location of the lesion.
However, it stands out the increase of the number of OSCC cases diagnosed from 1.64% (1998-2006) to 3.56% (2007-2019) of all cases received at the Oral Pathology Laboratory. These data show the evolution from 4.7 to 17.5 cases/year, probably reflecting an increased demand for consultation to the local population, which calls for professional qualification to improve the diagnosis of oral cancer. It is possible to infer that these results do not necessarily mean that the incidence of oral cancer has increased, but a higher number of patients was evaluated at the Service instead. On the other hand, the predominance of Grade II tumors (Table 2) remains through the whole period evaluated, which may indicate the need for improvement of the process of early diagnosis (Table 4).
Today, the tumor is more prevalent at the tongue and floor of the mouth instead of gingiva/alveolar ridge and palate, a clear tendency in its location. In addition, the quality of the description of the clinical aspect of the lesion has changed over the years: instead of ulcer/ulceration, there is significant presence of more specific descriptions such as infiltrative, superficial, or vegetative ulcer (Table 4). This change can be attributed to dentists’ improved skills for diagnostic process.
A study identified that approximately 12 years of education is a predictor protective factor for oral cancer, while risk factors were past or present use of alcohol, tobacco and previous diagnosis of cancer4,14. The delay in the process of oral cancer diagnosis may be associated with many factors involving the patients, the health system, and professionals. The lack of information and patients fear, in addition to several asymptomatic lesions are concerning2,21. Programs that aim to create strategies for awareness and education regarding risk factors such as tobacco and alcohol use, self-examination and symptoms of oral cancer are important tools as well1,5,7-9,13,14,21,22.
However, the existence of a healthcare system itself does not guarantee the diagnosis of oral cancer13 because health professionals need to be trained to identify potentially malignant lesions and cancer2,13,14,21. In addition, the medical consultation scheduling, the public transportation system, cultural and financial issues may cause delay2. Moreover, the information from geospatial analysis could be useful for policymakers in the implementation of place-specific control and preventive policies focused to high-risk populations13.
Therefore, the responsibility of a University as an Educational Institution for the community goes beyond its geographical localization. The Service has improved along its 22 years of existence with significant achievements as:
1) The number of local patients consulted increased significantly in this period and today, it represents almost half of the cases;
2) The staff of the Dental Clinic (Stomatology) increased, and a substantial number of biopsies were performed, and the Oral Pathology Laboratory received more biopsies from off-University dentists;
3) Dental students at the Federal University of Alfenas were extensively trained to detect and manage oral premalignant lesions during these past few years, which may possibly explain the increasing number of patients from SRS’ other than Alfenas’ (many undergraduate and graduate students start their practice on nearby towns). Moreover, the use of mobile phone applications and cameras ensure easy exchange of information among former and current students and the University staff;
4) Oral Medicine Professors offer training as continuing education for local health professionals;
5) The recent creation of an Institute of Oncology in the city of Alfenas strengthened the bond between the University and the regional population, possibly ensuring the early access to diagnosis and treatment of oral cancer.
CONCLUSION
In conclusion, the evolution of the Dental Clinic (Stomatology) and Oral Pathology Laboratory at the Federal University of Alfenas reinforces the importance of offering a specialized dental services in underserved regions through training and continuing education for local health professionals as well as improvement of the care network for early diagnosis and treatment of oral cancer.
CONTRIBUTIONS
Laura Cruz-Mamani contributed for the study design, methodology, original draft; Alessandro Antônio Costa Pereira, João Adolfo Costa Hanemann contributed for the study design; Marta Miyazawa contributed for the methodology, writing, review and editing; Denismar Alves Nogueira contributed for the methodology; Felipe Fornias Sperandio contributed for the methodology; João Adolfo Costa Hanemann for funding acquisition and supervision. All reviewed, read and approved the final version to be published.
CONFLICTS OF INTEREST
There is no conflict of interest to declare.
FUNDING
This study was funded by the National Council for Scientific and Technological Development (CNPq, Brazil): Grant/Award Number: 420698/2018-3; and Coordination for the Improvement of Higher Education Personnel (CAPES), Brazil), Grant/Award Number: Finance Code 001.
REFERENCES
1. Abdo EN, Garrocho AA, Barbosa AA, et al. Time elapsed between the first symptoms, diagnosis and treatment of oral cancer patients in Belo Horizonte, Brazil. Med Oral Patol Oral Cir Bucal. 2007;12(7):E469-73.
2. Santos LCO, Batista OM, Cangussu MCT. Characterization of oral cancer diagnostic delay in the state of Alagoas. Braz J Otorhinolaryngol. 2010;76(4):416-22. doi: https://doi.org/10.1590/S1808-86942010000400002
3. Martins Filho PRS, Santos TS, Silva LCF, et al. Oral cancer in Brazil: a secular history of public health policies. Rev Gaúch Odontol. 2014;62(2):159-64. doi: https://doi.org/10.1590/1981-8637201400020000091688
4. Ribeiro ILA, Nóbrega JBM, Valença AMG, et al. Predictors for oral cancer in Brazil. Rev Odontol UNESP. 2017;46(6):325-29. doi: https://doi.org/10.1590/1807-2577.06117
5. França GM, Silva LAB, Silva FMA, et al. Epidemiological profile of oral squamous cell carcinoma in a Northeastern Brazilian state. Arch Head Neck Surg. 2018;47(2):e910. doi: https://doi.org/10.4322/ahns.2018.0910
6. Paraguassu EC, Ramos PF, Oliveira LB, et al. Systematic review of the epidemiology of oral cancer in Brazil. Int J Innov Educ Res. 2019;7(4):366-74. doi: https://doi.org/10.31686/ijier.vol7.iss4.1431
7. Faria SO, Nascimento MC, Kulcsar MAV. Malignant neoplasms of the oral cavity and oropharynx treated in Brazil: what do hospital cancer records reveal? Braz J Otorhinolaryngol. 2020;S1808-8694(20)30089-6. doi: https://doi.org/10.1016/j.bjorl.2020.05.019
8. Wünsch-Filho V. The epidemiology of oral and pharynx cancer in Brazil. Oral Oncol. 2002;38(8):737-46. doi: https://doi.org/10.1016/S1368-8375(02)00066-0
9. Silva PGB, Mesquita KC, Dantas TS, et al. A ten-year retrospective study of the clinical, sociodemographic, and survival characteristics of patients with oral and pharyngeal squamous cell carcinomas. Braz J Health Rev. 2019;2(6):5160-72. doi: https://doi.org/10.34119/bjhrv2n6-022
10. Curado MP, Johnson NW, Kerr AR, et al. Oral and oropharynx cancer in South America: incidence, mortality trends and gaps in public databases as presented to the Global Oral Cancer Forum. Transl Res Oral Oncol. 2016;1:1-7. doi: https://doi.org/10.1177/2057178X16653761
11. Instituto Nacional de Câncer José Alencar Gomes da Silva. Estimativa 2020: incidência de câncer no Brasil. Rio de Janeiro: INCA; 2019.
12. Fonseca EP, Oliveira CDL, Chiaravalloti Neto F, et al. Bayesian model and spatial analysis of oral and oropharynx cancer mortality in Minas Gerais, Brazil. Ciênc Saúde Colet. 2018;23(1):153-60. doi: https://doi.org/10.1590/1413-81232018231.17022015
13. Soto AL, Sousa AA, Pinheiro LC, et al. Oral cancer: socio-spatial analysis of a Brazilian sample. Rev Bras Cancerol. 2020;66(3):e-061029. doi: https://doi.org/10.32635/2176-9745.RBC.2020v66n3.1029
14. Grossmann SMC, Sales ACR, Reis DS, et al. Knowledge of oral cancer by a Brazilian population. J Cancer Educ. 2021;36(5):965-70. doi: https://doi.org/10.1007/s13187-020-01722-4
15. Carli ML, Santos SL, Pereira AAC, et al. Características clínicas, epidemiológicas e microscópicas do câncer bucal diagnosticado na Universidade Federal de Alfenas. Rev Bras Cancerol. 2009;55(3):205-11. doi: https://doi.org/10.32635/2176-9745.RBC.2009v55n3.1608
16. El-Naggar AK, Chan JKC, Grandis JR, et al, editors. WHO Classification of head and neck tumours. 4th ed. Lyon (France): International Agency for Research on Cancer; 2017.
17. StataCorp [Internet]. Stata: release 16. Statistical software. College Station (TX): StataCorp LLC; c1996-2022 – [cited 2020 Oct 25]. Available from: https://www.stata-press.com/data/r16/
18. Secretaria de Estado de Saúde de Minas Gerais [Internet]. Belo Horizonte (MG): SES; [data desconhecida]. Superintendências Regionais de Saúde (SRS) e Gerências Regionais de Saúde (GRS); 2011 ago 2 [atualizado 2021 dez 6; acesso 2020 out 25]. Disponível em: https://saude.mg.gov.br/sobre/institucional/superintendencias-regionais-de-saude-e-gerencias-regionais-de-saude
19. Castro MC, Massuda A, Almeida G, et al. Brazil's unified health system: the first 30 years and prospects for the future. Lancet. 2019;394(10195):345-56. doi: https://doi.org/10.1016/S0140-6736(19)31243-7
20. Cunha AR, Prass TS, Hugo FN. Mortality from oral and oropharyngeal cancer in Brazil: impact of the National Oral Health Policy. Cad Saúde Pública. 2019;35(12):e00014319. doi: https://doi.org/10.1590/0102-311x00014319
21. Bandeira CM, Almeida AA, Carta CFL, et al. How to improve the early diagnosis of oral cancer? Braz Dent Sci. 2017;20(4):25-31. doi: https://doi.org/10.14295/bds.2017.v20i4.1439
22. Tomo S, Armelin AML, Hernandes ACP, et al. Oral lesions detected during a population screening for prevention and early diagnosis of oral cancer and potentially malignant disorders. RFO UPF. 2019;24(3):350-4. doi: https://doi.org/10.5335/rfo.v24i3.9818
Recebido em 22/11/2021
Aprovado em 21/2/2022
Associate Editor: Claudio Gustavo Stefanoff. Orcid iD: https://orcid.org/0000-0001-7050-3269
Scientific Editor: Anke Bergmann. Orcid iD: https://orcid.org/0000-0002-1972-8777
![]()
Este é um artigo publicado em acesso aberto (Open Access) sob a licença Creative Commons Attribution, que permite uso, distribuição e reprodução em qualquer meio, sem restrições, desde que o trabalho original seja corretamente citado.
©2019 Revista Brasileira de Cancerologia | Instituto Nacional de Câncer José Alencar Gomes da Silva | Ministério da Saúde