CASE REPORT
Pituitary Metastasis Clinical Presentation of Diabetes Insipidus Six Years after Invasive Breast Carcinoma Diagnosis: Case Report
Apresentação Clínica de Metástase Hipofisária com Diabetes Insipidus Seis Anos após o Diagnóstico de Carcinoma Mamário Invasivo: Relato de Caso
Presentación Clínica de Metástasis Hipofisaria con Diabetes Insípida Seis Años después del Diagnóstico de Carcinoma Mamario Invasivo: Informe de Caso
https://doi.org/10.32635/2176-9745.RBC.2023v69n4.4212
Samya Hamad Mehanna1; Julia Costa Linhares2; Emily Karoline Araujo Nonato Dos Santos3; Teresa Cristina Cavalcanti4
1,3Faculdade Evangélica Mackenzie do Paraná (Fempar). Curitiba (PR), Brazil. E-mails: samyahm88@gmail.com; emilynonatoaraujo@gmail.com. Orcid iD: https://orcid.org/0000-0002-6636-1314; Orcid iD: https://orcid.org/0000-0001-6671-4493
2,4Hospital Universitário Evangélico Mackenzie (HUEM), Departamento de Patologia. Curitiba (PR), Brazil. E-mails: juliaclinhares@yahoo.com.br; tecava@yahoo.com.br. Orcid iD: https://orcid.org/0000-0002-2651-0610; Orcid iD: https://orcid.org/0000-0002-8555-6547
Corresponding author: Emily Karoline Araujo Nonato dos Santos. Rua Padre Anchieta, 2770 – Bigorrilho. Curitiba (PR), Brazil. CEP 80730-000. E-mail: emilynonatoaraujo@gmail.com
ABSTRACT
Introduction: Breast carcinomas are the major cause of death in women with cancer worldwide, mainly in metastatic cases. The pituitary gland stands for only 6-8% of the secondary sites of distant metastasis and it is usually asymptomatic. When symptomatic, these lesions can mimic primary pituitary diseases. Case report: A 43-year-old woman underwent a left mastectomy with axillary lymph node dissection in April 2013 due to a luminal, invasive ductal carcinoma with nodal metastasis. Six years later, she started complaining of myalgia, bone pain, dizziness and decreased visual acuity, in addition to polydipsia and polyuria. Laboratory tests showed hyperprolactinemia and diabetes insipidus suggestive of panhypopituitarism. Magnetic resonance imaging of the brain showed a sellar tumor with extension to adjacent structures which was removed on November 2019. A pathology report of an epithelial neoplasm of unknown origin and an immunohistochemical study showed positivity for estrogen, progesterone receptors and GATA 3, and negativity for pituitary hormones. This set of findings and the histological morphology were consistent with a metastatic mucinous adenocarcinoma of mammary origin without HER-2 overexpression. The patient underwent ovarian ablation, central nervous system radiotherapy, chemotherapy and oncological follow-up. Conclusion: The patient's young age and clinical presentation of visual impairment and sudden development of diabetes insipidus diverges from the current data, since these findings are usually present in asymptomatic women over sixty-years-old. The varied clinical presentation can lead to a delay in diagnosis of pituitary metastasis, which reinforces the importance of reporting cases like this.
Key words: breast neoplasms; hypopituitarism; neoplasm metastasis.
RESUMO
Introdução: O carcinoma mamário é a maior causa de morte por câncer em mulheres no mundo, majoritariamente nos casos metastáticos. A hipófise configura apenas 6-8% dos sítios metastáticos a distância, e geralmente são assintomáticos. Quando sintomáticos, podem mimetizar uma doença primária dessa glândula. Relato do caso: Mulher, 43 anos, submetida à mastectomia com esvaziamento axilar à esquerda em abril de 2013 por carcinoma mamário ductal invasivo, luminal, com metástase linfonodal. Seis anos depois, iniciou com queixa de mialgia, dor óssea, tontura e piora progressiva de acuidade visual, além de polidipsia e poliúria. Exames laboratoriais evidenciaram hiperprolactinemia e diabetes insipidus sugerindo pan-hipopituitarismo. A ressonância magnética de encéfalo demonstrou tumor selar com extensão a estruturas adjacentes que foi ressecado em novembro de 2019, com laudo de neoplasia epitelial de origem indeterminada, sendo necessário estudo imuno-histoquímico para elucidação diagnóstica. Houve positividade para o receptor de estrógeno, progesterona e GATA 3 e negatividade para hormônios hipofisários. Esse conjunto de achados e a morfologia histológica foram condizentes com adenocarcinoma mucinoso metastático de origem mamária, sem hiperexpressão de HER-2. A paciente foi submetida à ablação ovariana, radioterapia em sistema nervoso central, quimioterapia e a acompanhamento oncológico. Conclusão: A idade, a apresentação clínica de comprometimento visual e o desenvolvimento de diabetes insipidus repentino destoam dos dados da literatura, uma vez que estes costumam estar associados a mulheres acima dos 60 anos e assintomáticas. Essa apresentação clínica diversificada pode levar a um atraso no diagnóstico da metástase hipofisária, o que reforça a importância de relatar casos como este.
Palavras-chave: neoplasias da mama; hipopituitarismo; metástase neoplásica.
RESUMEN
Introducción: Los carcinomas de mama son la principal causa de muerte en mujeres con cáncer en todo el mundo, principalmente en casos metastásicos. La glándula pituitaria representa solo el 6-8% de los sitios secundarios de metástasis a distancia y generalmente es asintomática. Cuando son sintomáticas, estas lesiones pueden imitar enfermedades pituitarias primarias. Informe de caso: Mujer, 43 años, se sometió a una mastectomía izquierda con disección de ganglios linfáticos axilares en abril de 2013 debido a un carcinoma de mama ductal invasivo luminal con metástasis ganglionar. Seis años después, comenzó a quejarse de mialgia, dolor óseo, mareos y disminución de la agudeza visual, además de polidipsia y poliuria. Los análisis de laboratorio revelaron hiperprolactinemia y diabetes insípida, lo que sugiere un cuadro de panhipopituitarismo. La resonancia magnética cerebral mostró un tumor de la silla turca con extensión a estructuras adyacentes, que se extirpó en noviembre de 2019. Un informe patológico indicó una neoplasia epitelial de origen desconocido, y ha sido necesario un estudio inmunohistoquímico para dilucidar, que se mostró positivo para los receptores de estrógeno, progesterona y GATA 3, y negativo para las hormonas pituitarias. Este conjunto de hallazgos y la morfología histológica fueron consistentes con un adenocarcinoma mucinoso metastásico de origen mamario sin superexpresión de HER-2. La paciente se sometió a ablación ovárica, radioterapia del sistema nervioso central, quimioterapia y seguimiento oncológico. Conclusión: La edad de la paciente y la presentación clínica de deterioro visual y desarrollo repentino de diabetes insípida difieren de los datos actuales, ya que estos hallazgos suelen estar presentes en mujeres asintomáticas mayores de 60 años. Una variada presentación clínica puede retrasar el diagnóstico de metástasis pituitaria, lo que refuerza la importancia de informar casos como este.
Palabras clave: neoplasias de la mama; hipopituitarismo; metástasis de la neoplasia.
INTRODUCTION
In 2023, breast cancer was the most diagnosed cancer in Brazil, excluding nonmelanoma skin cancers, accounting for approximately 41.89 cases per 100,000 women1,2. More than 2.26 million new cases of breast cancer were diagnosed in women in 20203 worldwide. Of all the breast malignancies, 95% are carcinomas of epithelial origin, the most frequent are nonspecific invasive carcinomas, subclassified according to immunohistochemical (IHC) in relation to positivity or lack thereof of the following markers: estrogen receptor (ER), progesterone receptor (PR) and human epidermal growth factor receptor (HER-2) type 2. These are prognostic markers that can define the course of the treatment4.
Metastatic breast carcinoma is the main factor contributing to mortality in these types of cancers. They primarily spread through the bloodstream, leading to the development of metastases in various organs, including the brain and bones. Central nervous system (CNS) metastases are frequently associated with worse prognosis since they are less responsive to systemic therapies5.
The pituitary is a highly vascularized gland located in the sellar region and neoplasms at these sites account for approximately 15% of all brain tumors6. It is estimated that about 6 to 8% of breast cancer cases affect this gland, but they are challenging to diagnose and treat7,8.
Due to few cases reported in medical literature, the poor outcome of a late diagnosis and the necessity to shed light on the diagnosis, the objective of this study is to describe a case of pituitary metastasis of breast carcinoma six years after the primary treatment of a young patient at a philanthropic university hospital in Curitiba, State of Paraná.
The Institutional Review Board (IRB) of “Faculdade Evangélica Mackenzie” in Curitiba, Paraná approved the study, report number 4,166,895, CAAE ( submission for ethical review) number 34032120.2.0000.0103, in compliance with Resolution 466/20129 of the National Health Council.
CASE REPORT
In July 2012, a 37-year-old female patient underwent an ultrasound (US)-guided core needle left breast biopsy due to a suspicious mammogram result with microcalcifications and focal asymmetry and distortion classified as BIRADS 4C in February of the same year. The biopsy results revealed an invasive ductal carcinoma, luminal A; clinically, the patient presented with nipple retraction and a 4.0 cm lump on the left breast, she was prescribed a neoadjuvant chemotherapy with doxorubicin hydrochloride, cyclophosphamide and paclitaxel from 12th September, 2012 to 28th February, 2013. In April 2013, the patient submitted to left mastectomy with axillary lymph node dissection, the pathological staging was pT3 pN1 due to the tumor dimensions and nodal involvement. The patient was prescribed adjuvant radiotherapy (from December 2013 to February 2014) and tamoxifen 20 mg daily after the surgery.
She was referred to a tertiary hospital in April 2019 for diagnostic curettage in order to seek the cause of an endometrial thickening – later diagnosed as endometrial hyperplasia secondary to the use of tamoxifen. In October of the same year she started complaining of generalized myalgia and bone pain, dizziness with occasional episodes with syncope, and progressive worsening of visual acuity, in addition to polydipsia and polyuria. Computerized tomography (CT) scan (Figure 1) and magnetic resonance imaging (MRI) results showed an expansive lesion in the sellar and suprasellar regions with a compressive effect on the optic chiasm. Laboratory tests showed hyperprolactinemia and panhypopituitarism suggestive of diabetes insipidus.
|
|
|
Figure 1. Computerized tomography scan showing an expansive lesion in the sellar and suprasellar regions |

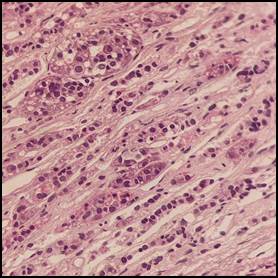
The first diagnostic hypothesis was of a pituitary macroadenoma, and the patient was referred to endocrinology sector. In November of the same year the tumor was resected via a transsphenoidal surgery, and after the anatomical pathology analysis of the specimen collected, a diagnosis of epithelial neoplasm of unknown origin was reached (Figure 2).
|
|
|
Figure 2. Light microscopy demonstrated pleomorphic cell groupings suggestive of an epithelial neoplasm of unknown origin |
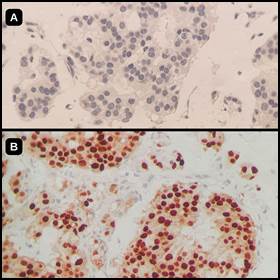
IHC results showed positivity for estrogen (Figure 3) and progesterone receptors and GATA3 and negativity for pituitary hormones (ACTH, FSH, LH, TSH, GH and prolactin) (Figure 3). With this set of findings (patient history, tumor location, histological morphology and IHC markers) the final diagnosis was of a metastatic mucinous adenocarcinoma mammary in origin with HER-2 weakly and coarsely reactive, classified as negative (Score 1+).
|
|
|
Figure 3. Immunohistochemical results showed negativity for pituitary hormones (ACTH, FSH, LH, TSH, GH and prolactin), as demonstrated by the absent reaction at (A) (prolactin) and positivity for estrogen (B) and progesterone receptors and GATA3 |
The bone pain was due to spinal metastatic foci and a leptomeningeal metastasis was also detected. The patient underwent ovarian ablation, CNS radiotherapy, palliative chemotherapy with capecitabine and oncological and palliative care (pain outpatient clinic). During follow up in 2021, the patient presented with diarrhea, nausea and vomiting which was attributed to capecitabine-related toxicity. She experienced hemodynamic instability and dyspnea, likely resulting from bronchoaspiration and passed away a few days later due to refractory shock.
DISCUSSION
Cancer at the pituitary gland resulting from metastasis predominantly occurs in patients over 60-years-old, with lungs and breast being the most common primary sites of origin10. Usually, patients with involvement of this gland do not experience any noticeable symptoms. However, in cases where symptoms do manifest and are present, diabetes insipidus is the prevalent form of manifestation. Other symptoms include anterior hypopituitarism, vision loss and CNS disorders7.
Pituitary metastases (PM) most commonly arise from breast cancer. In a recent systematic review of the literature with 32 studies and 38 patients, 62% of those with PM had diabetes insipidus as clinical manifestation11. For comparative purposes, a total of 41 (100%) reported cases of PM in women were compiled from the literature, with mean age of 58.8 ± 4.8 (range 30-91) years, mean time from primary diagnosis and metastasis of 6.8 ± 2.7 years and 35 (85.3%) cases (available data) of hormonal dysfunction (LH – luteinizing hormone, FSH – follicle-stimulating hormone, TSH – thyroid-stimulating hormone, Prolactin and/or GH – growth hormone) including those from the aforementioned systematic review conducted by Rasiah et al.11-14.
As symptoms are nonspecific of any type of lesion, further tests must be performed in order to have a clearer diagnosis5. Since imaging tests tend to vary and sometimes can be atypical, surgically obtained tissue samples and its subsequent histopathological and IHC analysis are usually necessary15.
Histological morphology tends to help but today IHC and molecular biology studies support the diagnosis as well. For instance, when facing a poorly differentiated neoplasm located in the sellar region, it is of utmost importance to differentiate primary pituitary from secondary (metastatic) neoplasms. IHC studies are not only useful to diagnose but are extremely helpful for a patient-centered treatment10.
On average, approximately 65% of the patients with PM have had other early metastatic lesions, bone metastasis being the most common. The time interval between breast carcinoma diagnosis and PM is 5 to 7 years11.
Like other types of carcinoma, the prognosis of breast carcinomas is deeply influenced by the patient's age, tumor histological grade and tumor staging at diagnosis13. Metastatic mammary carcinomas bear a similar immunoexpression to those found primarily in the breast showing positivity to epithelial markers and GATA-3, and variability positivity to hormone receptors (estrogen and progesterone). HER-2 overexpression can also be evaluated. Hormonal IHC markers such as ACTH, GH, Prolactin, TSH, FSH and LH, hormones produced in the pituitary gland tend to indicate this site as the origin of the lesion16,17. Approximately 30% of the cases evolve to death in an average time of seven months after the diagnosis of PM11.
Surgical removal, radiosurgery, chemotherapy and hormonal therapy are some of the treatments available and to date there are no standard treatment protocols. Some tumor characteristics, as well as patient performance status, can be challenging to complete surgical resection5,17. Recently, it is being observed that those who underwent adjuvant therapies (chemotherapy or chemotherapy in association with radiotherapy) had better survival rate than patients who undergo single surgical resection11.
CONCLUSION
Considering that the late diagnosis of pituitary metastasis can have dismal consequences on the prognosis and quality-of-life of the patient, the early and differential diagnosis of primary pituitary neoplasms in patients with breast cancer years after the initial diagnosis is very important.
CONTRIBUTIONS
All authors contributed substantially to the study design, acquisition, analysis, and interpretation of the data, wording and critical review. They approved the final version to be published.
DECLARATION OF CONFLICT OF INTERESTS
There is no conflict of interests to declare.
FUNDING SOURCES
None.
REFERENCES
1. Santos MO, Lima FCS, Martins LFL, et al. Estimativa de incidência de câncer no Brasil, 2023-2025. Rev Bras Cancerol. 2023;69(1):e-213700. doi: https://doi.org/10.32635/2176-9745.RBC.2023v69n1.3700
2. International Agency for Research on Cancer; World Health Organization [Internet]. Lyon: IARC; 2020. Cancer today. [date unknown]. [cited 2020 Nov 2] Available from: https://gco.iarc.fr/today/home
3. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209- 49. doi: https://doi.org/10.3322/caac.21660
4. Rocha ZH, Manica GCM, Noronha L, et al. Análise comparativa do perfil histopatológico e epidemiológico dos carcinomas ductal e lobular da mama diagnosticados no Hospital de Clínicas da Universidade Federal do Paraná entre 2008 e 2013. J Bras Patol Med Lab. 2019;55(1):69-86. doi: https://doi.org/10.5935/1676-2444.20190009
5. Watase C, Shiino S, Shimoi T, et al. Breast cancer brain metastasis-overview of disease state, treatment options and future perspectives. Cancers (Basel). 2021;13(5):1078. doi: https://doi.org/10.3390/cancers13051078
6. World Health Organizatin. Classification of tumours editorial board. endocrine and neuroendocrine tumours [Internet]. 5 ed. Lyon: International Agency for Research on Cancer; 2022 (Classification of tumours series, vol. 8). [cited 2020 Nov 2]. Available from: https://tumourclassification.iarc.who.int/chapters/36
7. Fortunati N, Felicetti F, Donadio M, et al. Pituitary lesions in breast cancer patients: A report of three cases. Oncol Lett. 2015;9(6):2762-6. doi: https://doi.org/10.3892/ol.2015.3149
8. Niikura N, Hayashi N, Masuda N, et al. Treatment outcomes and prognostic factors for patients with brain metastases from breast cancer of each subtype: a multicenter retrospective analysis. Breast Cancer Res Treat. 2014;147(1):103-12. doi: https://doi.org/10.1007/s10549-014-3090-8
9. Conselho Nacional de Saúde (BR). Resolução n° 466, de 12 de dezembro de 2012. Aprova as diretrizes e normas regulamentadoras de pesquisas envolvendo seres humanos. Diário Oficial da União, Brasília, DF. 2013 jun 13; Seção I:59.
10. Oueslati I, Ayari S, Yazidi M, et al. Hypopituitarism secondary to a pituitary metastasis in a young woman with an invasive breast carcinoma. Clin Case Rep. 2021;9(6):e04175. doi: https://doi.org/10.1002/ccr3.4175
11. Rasiah NP, Albakr A, Kosteniuk S, et al. Early and isolated breast cancer metastasis to the pituitary: a case report and systematic review. Surg Neurol Int. 2022;(13):462. doi: https://doi.org/10.25259/SNI_1053_2021
12. Minami K, Ueno Y, Minamidate Y, et al. A case of pituitary metastasis discovered when diabetes insipidus developed in a patient 20 years after breast cancer treatment. Radiol Case Rep. 2023;18(11):3904-7. doi: https://doi.org/10.1016/j.radcr.2023.08.025
13. Oueslati I, Ayari S, Yazidi M, et al. Hypopituitarism secondary to a pituitary metastasis in a young woman with an invasive breast carcinoma. Clin Case Rep. 2021;9(6):e04175. doi: https://doi.org/10.1002/ccr3.4175
14. Parthasarathy S, Lee DH, Levitt AH, et al. Pituitary metastasis presenting with central diabetes insipidus and panhypopituitarism. AACE Clin Case Rep. 2021;8(1):15-8. doi: https://doi.org/10.1016/j.aace.2021.06.006
15. Cai H, Liu W, Feng T, et al. Clinical presentation and pathologic characteristics of pituitary metastasis from breast carcinoma: cases and a systematic review of the literature. World Neurosurg. 2019;124:445-51. doi: https://doi.org/10.1016/j.wneu.2018.12.126
16. World Health Organiation. Classification of tumours editorial board. breast tumours [Internet]. 5 ed. Lyon: International Agency for Research on Cancer; 2019. (Classification of tumours series. vol. 2). [cited 2020 Nov 2]. Available from: https://tumourclassification.iarc.who.int/chapters/32
17. Komninos J, Vlassopoulou V, Protopapa D, et al. Tumors metastatic to the pituitary gland: case report and literature review. J Clin Endocrinol Metab. 2004;89(2):574-80. doi: https://doi.org/10.1210/jc.2003-030395
Recebido em 7/7/2023
Aprovado em 25/9/2023
Scientific-Editor: Anke Bergmann. Orcid iD: https://orcid.org/0000-0002-1972-8777
![]()
Este é um artigo publicado em acesso aberto (Open Access) sob a licença Creative Commons Attribution, que permite uso, distribuição e reprodução em qualquer meio, sem restrições, desde que o trabalho original seja corretamente citado.
©2019 Revista Brasileira de Cancerologia | Instituto Nacional de Câncer | Ministério da Saúde