ORIGINAL ARTICLE
Evaluation of Synthesized 2D Mammography Combined with Tomosynthesis: A Potential Approach to Reduce Radiation Exposure in Breast Cancer Diagnostic Exams
Avaliação da Mamografia 2D Sintetizada Combinada com Tomossíntese: Uma Abordagem Potencial para Reduzir a Exposição à Radiação em Exames de Diagnóstico de Câncer de Mama
Evaluación de la Mamografía 2D Sintetizada Combinada con Tomosíntesis: Un Enfoque Potencial para Reducir la Exposición a la Radiación en los Exámenes de Diagnóstico de Cáncer de Mama
https://doi.org/10.32635/2176-9745.RBC.2026v72n1.5470
Paula Medina Maciel Gomes Curi Bonotto1; Léonie Marie Catherine Lefebvre2; Carlos Frederico Motta Vasconcelos3; Antonio Mauricio Ferreira Leite Miranda de Sá4; Suzana Sales de Aguiar5; Anke Bergmann6
1Instituto Nacional de Câncer (INCA). Rio de Janeiro (RJ), Brasil. E-mail: paulamedinamg@gmail.com. Orcid iD: https://orcid.org/0009-0005-7989-8638
2Université de Rouen Normandie. Rouen, Normandia, França. E-mail: leonie.lef@gmail.com. Orcid iD: https://orcid.org/0009-0009-4816-717X
3INCA, Coordenação de Administração Geral (Coage), Serviço de Engenharia Clínica (Seclin). Rio de Janeiro (RJ), Brasil. E-mail: carlos.vasconcelos@inca.gov.br. Orcid iD: https://orcid.org/0009-0002-7947-9116
4Universidade Federal do Rio de Janeiro (UFRJ), Instituto Alberto Luiz Coimbra de Pós-Graduação e Pesquisa de Engenharia (Coppe). Rio de Janeiro (RJ), Brasil. E-mail: amflms@peb.ufrj.br. Orcid iD: https://orcid.org/0000-0001-8114-7255
5,6INCA, Coordenação de Pesquisa Clínica, Divisão de Pesquisa Clínica e Desenvolvimento Tecnológico. Rio de Janeiro (RJ), Brasil. E-mails: saguiar@inca.gov.br; abergmann@inca.gov.br. Orcid iD: https://orcid.org/0000-0003-1963-1294; Orcid iD: https://orcid.org/0000-0002-1972-8777
Corresponding author: Carlos Frederico Motta Vasconcelos. Seclin/Coage/INCA. Rua Marquês de Pombal, 125, 10º andar – Centro. Rio de Janeiro (RJ), Brasil. CEP 20230-240. E-mail: carlos.vasconcelos@inca.gov.br
ABSTRACT
Introduction: Breast cancer is the most common globally among the female population. Conventional 2D Full-Field Digital Mammography (FFDM) is the standard screening tool but limited in dense breasts. Digital Breast Tomosynthesis (DBT) reduces this limitation, especially in extremely dense and heterogeneously dense breasts; however, its routine combination with FFDM increases radiation exposure. Synthesized 2D Mammography (S2D) has been proposed as alternative to replace FFDM, reducing dose while maintaining diagnostic performance. Objective: Validate S2D as replacement for FFDM in breast cancer diagnostic to reduce radiation dose without compromising diagnostic accuracy. Method: Patients with suspected breast lesions have been evaluated at the National Cancer Institute (INCA). Images were obtained using combined protocol (FFDM+DBT), and S2D images were generated from DBT. Agreement between FFDM and S2D was assessed using Cohen´s Kappa. Diagnostic accuracy, sensitivity, and specificity of each imaging modality and their combinations were compared with percutaneous biopsy results. Results: Of the 149 patients included in this study, 75% had either dense or extremely dense breast tissue. Synthesized 2D showed excellent agreement with FFDM in lesion detection (κ= 0.757) and classification (κ= 0.867). DBT achieved 100% sensitivity for malignant lesions. The S2D+DBT combination demonstrated accuracy of 98.6% and sensitivity of 100%, comparable to FFDM+DBT but with 47.8% reduction in radiation dose. Conclusion: Synthesized 2D mammography is a reliable alternative to FFDM. Combined with DBT, S2D also provides accurate detection while significantly reducing radiation exposure, supporting its integration into breast cancer screening protocols, particularly in resource-constrained healthcare systems.
Key words: Mammography/instrumentation; Breast Neoplasms/diagnostic imaging; Early Detection of Cancer; Mass Screening.
RESUMO
Introdução: O câncer de mama é o mais comum entre a população feminina, com taxas de incidência crescentes no Brasil. O diagnóstico precoce é imperativo para um tratamento eficaz. A mamografia digital de campo total 2D convencional (Full-Field Digital Mammography – FFDM) é a ferramenta de rastreamento padrão, mas é limitada em mamas densas. A tomossíntese digital de mama (Digital Breast Tomosynthesis – DBT) reduz essa limitação, especialmente em mamas extremamente densas e mamas heterogeneamente densas; porém, sua combinação rotineira com a FFDM aumenta a exposição à radiação. A mamografia 2D sintetizada (Synthesized 2D Mammography -S2D) foi proposta como uma alternativa para substituir a FFDM, reduzindo dose e mantendo desempenho diagnóstico. Objetivo: Validar a S2D como substituta da FFDM no diagnóstico do câncer de mama para reduzir a dose de radiação sem comprometer a precisão diagnóstica. Método: Foram avaliadas pacientes com lesões mamárias suspeitas no Instituto Nacional de Câncer, Brasil. As imagens foram obtidas usando um protocolo combinado (FFDM+DBT), e as imagens S2D foram geradas a partir da DBT. A concordância entre FFDM e S2D foi avaliada usando Kappa-Cohen. A acurácia, sensibilidade e especificidade diagnósticas de cada modalidade de imagem e suas combinações foram comparadas com resultados da biópsia percutânea. Resultados: Das 149 pacientes incluídas neste estudo, 75% apresentavam tecido mamário denso ou extremamente denso. A S2D mostrou excelente concordância com a FFDM na detecção (κ=0,757) e classificação (κ=0,867) de lesões. A DBT alcançou sensibilidade de 100% para lesões malignas, incluindo quatro detectadas exclusivamente por DBT. A combinação S2D+DBT demonstrou acurácia de 98,6% e sensibilidade de 100%, comparável à FFDM+DBT, com redução de 47,8% na dose de radiação. Conclusão: S2D é uma alternativa confiável à FFDM. Combinada com DBT, S2D proporciona uma detecção precisa, enquanto reduz significativamente a exposição à radiação, apoiando sua integração em protocolos de rastreamento do câncer mamário, particularmente em sistemas de saúde com recursos limitados.
Palavras-chave: Mamografia/instrumentação; Neoplasias da Mama/diagnóstico por imagem; Detecção Precoce de Câncer; Programas de Rastreamento.
RESUMEN
Introducción: El cáncer de mama es el más común a nivel mundial entre la población femenina, con tasas de incidencia crecientes en el Brasil. El diagnóstico temprano es imperativo para un tratamiento eficaz. La mamografía digital de campo completo 2D convencional (Full-Field Digital Mammography – FFDM) es la herramienta de detección estándar, pero está limitada en mamas densas. La tomosíntesis digital de mama (Digital Breast Tomosynthesis – DBT) reduce esta limitación, especialmente en mamas extremadamente densas y mamas heterogéneamente densas; sin embargo, su combinación rutinaria con FFDM aumenta la exposición a radiación. La mamografía 2D sintetizada (Synthesized 2D Mammography - S2D) ha sido propuesta como una alternativa para reemplazar a la FFDM, reduciendo la dosis mientras mantiene el rendimiento diagnóstico. Objetivo: Validar la S2D como reemplazo de FFDM en el diagnóstico del cáncer de mama para reducir la dosis de radiación sin comprometer la precisión diagnóstica. Método: Se evaluó a pacientes con lesiones mamarias sospechosas en el Instituto Nacional del Cáncer, Brasil. Las imágenes se obtuvieron utilizando un protocolo combinado (FFDM+DBT), y las imágenes S2D se generaron a partir de los datos de DBT. La concordancia entre FFDM y S2D se evaluó usando el Kappa de Cohen. La precisión, la sensibilidad y la especificidad diagnósticas de cada modalidad de imagen y sus combinaciones se compararon luego con los resultados de la biopsia percutánea. Resultados: De las 149 pacientes incluidas en este estudio, el 75% tenía tejido mamario denso o extremadamente denso. La S2D mostró una excelente concordancia con FFDM tanto en detección (κ=0,757) como en clasificación (κ=0,867) de lesiones. La DBT logró una sensibilidad del 100% para lesiones malignas, incluyendo cuatro detectadas exclusivamente por DBT. La combinación S2D+DBT demostró una precisión del 98,6% y una sensibilidad del 100%, comparable a FFDM+DBT, pero con una reducción del 47,8% en la dosis de radiación. Conclusión: La S2D es una alternativa confiable a la FFDM. Combinada con la DBT, proporciona una detección precisa mientras reduce significativamente la exposición a radiación, apoyando su integración en los protocolos de detección del cáncer de mama, particularmente en sistemas de salud con recursos limitados.
Palabras clave: Mamografía/instrumentación; Neoplasias de la Mama/diagnóstico por imagen; Detección Precoz del Cáncer; Tamizaje Masivo.
INTRODUCTION
Breast cancer is the most common malignancy among women worldwide, with an estimated 2.3 million new cases and 670,000 deaths reported in 20221. In Brazil, breast cancer accounts for nearly one-third of all female cancers, with 73,610 new cases projected for 2023–2025, corresponding to an incidence of 41.9 per 100,000 women2. The growing incidence underscores the critical importance of early and accurate detection, which improves treatment outcomes and reduces mortality. However, mortality rates vary considerably across regions, reflecting disparities in access to healthcare resources and imaging technologies3.
Presently, full-field digital mammography (2D FFDM) is the standard method for breast cancer screening3. However, conventional 2D FFDM presents some limitations, especially in women with dense breasts, where the superposition of anatomical structures in the final image can mask lesions4,5. To improve the interpretation of images and their quality, new technologies have been developed. One such technology is digital breast tomosynthesis (DBT), which shows breast tissue in three dimensions, facilitating the detection, location, and characterization of lesions4.
Nevertheless, one issue that may limit the use of DBT is the difficulty in detecting calcifications, which may be better seen on 2D FFDM. Consequently, in clinical practice, DBT is frequently combined with FFDM (the "Combo" protocol), which increases the patient's radiation dose5. At the National Cancer Institute (INCA), patients often present for their initial consultation with previous medical examinations from other centers, many of which were performed under precarious and inadequate technical conditions. For a proper evaluation, it is often necessary to perform new images, which expose the patient to additional radiation. It is imperative to note that the breast is a radiosensitive organ. Consequently, it is essential to limit the total radiation dose in order to ensure patient safety6.
Synthesized 2D mammography (S2D) is an imaging technology where a 2D image is reconstructed from 3D DBT images, aiming to replace conventional FFDM without the use of radiation during its creation. Synthesized mammography (S2D) offers certain advantages including reduced radiation exposure and a reduced examination time compared to FFDM. In addition, it has been shown to maintain or even improve performance in breast lesion detection. However, because each manufacturer may utilize distinct algorithms and processing techniques to generate tomosynthesis and synthesized mammography images, it is observed that each equipment model can produce images with different levels of quality4.
Despite its availability at institutions like INCA (National Cancer Institute) since 2017, Digital Breast Tomosynthesis (DBT) is offered by only a few public centers in Brazil. This disparity creates significant challenges, marked by resource constraints and unequal access to advanced image diagnostic tools. To overcome these barriers, validating efficient and lower-dose image diagnostic protocols is a priority. The objective of this study was to assess whether S2D could replace FFDM in combination with DBT, thereby simplifying breast imaging protocols and reducing patient radiation exposure without compromising diagnostic accuracy.
METHOD
The study was based on data and images collected at INCA's “Hospital do Câncer III (HC3/INCA)” between April 1st and September 30th, 2019. Patients who attended the institution with pre-existing complaints, for further clarification, underwent diagnostic tests, which were included in this study. All participants provided informed consent prior to enrollment.
The equipment selected for this study was a Selenia Dimensions 3D mammography machine (Hologic). The conventional "Combo" protocol was used to collect and generate images for each patient, consisting of an initial 3D digital tomosynthesis (DBT) exam, followed by a 2D digital mammography (FFDM) exam, utilizing a single breast compression. Synthesized mammography (S2D) images were generated from the DBT images using the C-View/Hologic software (version 2019).
All mammograms were performed in craniocaudal (CC) and mediolateral oblique (MLO) views. Still, if necessary, at the time of the appointment, additional views were performed according to radiological demand, such as the 90-degree profile, magnification, spot compression, exaggerated craniocaudal, rolled, tangential, axillary prolongation, "cleavage", and "eklund".
Synthesized mammography images were compared with those obtained by conventional FFDM and tomosynthesis (DBT) using Cohen's Kappa index, calculated to evaluate the agreement between the results of the different imaging modalities.
An analysis of the diagnostic performance of each imaging modality was also performed relative to the results of histopathological biopsies, which are considered the gold standard for cancer diagnosis. The sensitivity, specificity, and accuracy were calculated.
Moreover, the radiation doses emitted by the mammograph X-ray tube in mediolateral oblique (MLO) and craniocaudal (CC) incidences were quantified as Entrance Surface Air Kerma (ESAK, mGy) using DICOM metadata files. The total radiation doses for each technique were then compared to determine whether the use of synthesized mammography would allow for a significant reduction in X-ray exposure without compromising the diagnostic quality and reliability.
Three imaging modalities were compared:
● Conventional 2D Mammography (FFDM): This is the most widely used method on a global scale. It is the preferred tool for breast cancer screening. It produces 2D images that allow the analysis of the breast and the identification of potential abnormalities. However, this technology has limitations related to superimposed structures, which can make it difficult to locate and differentiate lesions4,5.
● 3D Digital Tomosynthesis (DBT): Tomosynthesis facilitates the acquisition of multiple low-dose radiographic projections of the breast performed at different angles. The images are then reconstructed into a pseudo-three-dimensional volume4. This technique provides better visibility of breast lesions, especially in dense breasts, particularly by reducing tissue superposition. In addition, 3D mammography has improved sensitivity over 2D mammography, allowing for better detection of masses and architectural distortion.
● C-View (synthesized mammography images (S2D) reconstructed from DBT data): This is a technology that allows the synthesis and reconstruction of 2D mammography images (S2D) from DBT images using specific software7. This technique has been validated by the US FDA (Food and Drug Administration) since May 20138.
The results of the following combinations of imaging modalities were also compared:
● FFDM and DBT Combination (Standard "Combo" Protocol)
● S2D and DBT Combination
To collect information for subsequent analysis, a specific form was created. This tool allows the medical professional to transcribe the data more easily.
Demographic data (age, race/ethnicity, body mass index – BMI), clinical variables, and imaging findings were recorded using a standardized form (supplementary material). Lesions were characterized by number, laterality, topographic location, and imaging features, including morphology and distribution of calcifications, nodule shape and margins, asymmetries, and architectural distortions. Histopathological results were retrieved from electronic medical records when biopsy was performed, including tumor type, grade, and receptor status (ER, PR, HER2, Ki-67).
Breast density was evaluated by INCA’s radiologists and documented in the medical reports. This assessment of the proportion of heterogeneously dense and extremely dense breasts versus predominantly fatty breasts and breasts with sparse fibroglandular tissue is essential to interpreting the results, as higher density breasts can mask small cancers and is also independently associated with an increased risk of developing breast cancer.
The calculation of Cohen’s Kappa coefficient (κ) is determined by the following formula:
κ=(Po−Pe)/(1−Pe)
where:
● Po is the observed proportion of agreement. It is the number of cases where the two imaging exams agree, divided by the total number of cases.
● Pe is the proportion of agreement expected by chance. It is the probability that the imaging exams agree randomly, considering the marginal distributions of the classifications of each method.
Cohen’s Kappa coefficient (κ) was used to assess inter-modality agreement for lesion detection and classification among FFDM, S2D, and DBT, as well as for combined protocols ([FFDM + DBT] vs. [S2D + DBT]). Agreement was interpreted according to Fleiss’ criteria9: poor (≤0.40), fair (0.41–0.59), good (0.60–0.74), and excellent (≥0.75).
Diagnostic performance was evaluated against histopathology (gold standard) by calculating sensitivity, specificity, and accuracy for each image modality and combined protocols.
The accuracy index measures the total proportion of correct classifications of the imaging exam (both true positives and true negatives). Accuracy is calculated over the total number of cases and provides a general measure of the performance of imaging exams.
Accuracy = (TP+TN)/(Total Number of Cases)
where TP = True Positive – cases where the lesion was identified and the biopsy result was malignant, while TN = True Negative – cases where the lesion was identified and the biopsy result was benign.
Next, the sensitivity index measures the ability of the imaging exam to correctly identify lesions with a biopsy result of malignancy (i.e., a condition or disease, or true positives) as shown below:
Sensitivity = TP/(TP+FN)
where TP = True Positive – cases where the lesion was identified and the biopsy result was malignant, and FN = False Negative – cases where the lesion was not identified and the biopsy result was malignant.
Therefore, sensitivity indicates the proportion of cases with malignant lesions that were correctly identified by the imaging exam.
Specificity index measures the ability of the imaging exam to correctly identify lesions with a biopsy result of benignity (i.e., without a condition or disease, or true negatives) as follows:
Specificity = TN/(TN+FP)
where TN = True Negative – cases in which the identified lesion was not suspected and the biopsy result was benign, while FP = False Positive – cases in which the injury was identified as suspicious and the biopsy result was benign.
Specificity is employed to denote the proportion of cases with benign lesions that were correctly identified by the imaging exam.
Finally, radiation dose emitted by the X-ray tube in mediolateral oblique and craniocaudal incidences was quantified as Entrance Surface Air Kerma (ESAK, mGy) from DICOM metadata files. Results were reported with 95% confidence intervals.
INCA’s Research Ethics Committee approved the study on April 2, 2020 (CAAE (submission for ethical review) 04638818.4.0000.5274) and approval report number 3122074 in compliance with Directive 466/201210 of the National Health Council.
RESULTS
A total of 149 patients, already with previous clinical complaints or previous tests showing suspicious changes, were included, resulting in the detection of 220 breast lesions, submitted to percutaneous mammography or ultrasound-guided biopsies (core biopsy, vacuum-assisted biopsy, or tru-cut). Histopathological analysis revealed that 36.9% of the patients had only benign lesions, while 63.1% had at least one malignant lesion. Among patients with a malignant lesion, 25.5% were under 50 years old, and among all patients with any lesion, 34.9% were under 50 years old (Table 1).
Regarding breast density evaluation, about 75% of the patients in this study presented with either heterogeneously dense and extremely dense breasts. The remaining patients showed less dense classifications, with approximately 15% having scattered areas of fibroglandular density and less than 10% presenting with almost entirely fatty breasts. As will be seen, this information is relevant due to the importance of DBT in detecting cancer in high-density tissue.
Table 1. Number of patients with breast lesions by age group
|
Age |
Less than 50 years N (%) |
50 or more years N (%) |
Total N (%) |
|
Patients with only benign lesion |
14 (9.4) |
41 (27.5) |
55 (36.9) |
|
Patients with at least one malignant lesion |
38 (25.5) |
56 (37.6) |
94 (63.1) |
|
Total |
52 (34.9) |
97 (65.1) |
149 (100) |
Agreement in lesion detection
Cohen’s Kappa analysis showed excellent statistical agreement between FFDM and S2D for lesion detection (κ = 0.757). In contrast, DBT exhibited lower agreement with both FFDM (κ = 0.224) and S2D (κ = 0.212). This lower statistical agreement is expected but does not imply inferior diagnostic performance as it primarily reflects the fundamental modality differences between a single 2D projection (FFDM or S2D) and a multi-slice 3D volume (DBT). In fact, DBT's ability to separate overlapping tissues and reveal subtle lesions not visible on a single 2D projection inherently changes the determination of 'present' or 'absent' lesion locations, thus leading to a lower statistical agreement with the 2D images. When evaluating combined protocols, [FFDM + DBT] and [S2D + DBT] demonstrated good statistical agreement (κ = 0.662).
Agreement in lesion classification
For lesion classification (distortions, microcalcifications, asymmetries, and architectural distortions), agreement between FFDM and S2D was excellent (κ = 0.867). DBT showed good agreement with FFDM (κ = 0.677) and S2D (κ = 0.682). Combined protocols also achieved excellent concordance ([FFDM + DBT] vs. [S2D + DBT]: κ = 0.764).
Diagnostic performance in comparison with biopsy
When compared with biopsy (gold standard), DBT detected all 103 malignant lesions, yielding 100% sensitivity.
Ten lesions, including four malignancies, were identified exclusively by DBT. Since these lesions were found in patients with dense or extremely dense breasts, this result emphasizes the importance of DBT in detecting cancer in high-density tissue. One benign asymmetry was detected only by FFDM, and another by S2D.
The combination of S2D with DBT achieved accuracy of 98.6%, sensitivity of 100%, and specificity of 97.4%, comparable to the conventional FFDM + DBT protocol (Table 2).
Table 2. Accuracy, sensitivity, and specificity results of imaging modalities in relation to biopsy results
|
Indexes |
Biopsy versus FFDM % |
Biopsy versus S2D (C-View) % |
Biopsy versus DBT (Tomo 3D) % |
Biopsy versus Combo (DBT+S2D) % |
|
Sensitivity |
95.1 |
94.2 |
100 |
100 |
|
Specificity |
91.5 |
91.5 |
93.2 |
97.4 |
|
Accuracy |
93.2 |
92.7 |
96.4 |
98.6 |
Synthesized S2D (C-View) demonstrated adequate visualization of calcifications when compared with conventional FFDM, with similar accuracy in identifying calcifications in both tests (Figure 1). DBT improved margin definition of breast nodules relative to 2D Imaging, as demonstrated in this case of a suspicious nodule (Figure 2).
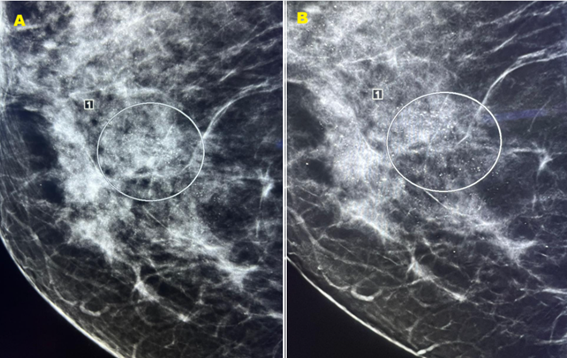
Figure 1. Conventional 2D FFDM mammography image with identification of amorphous and segmental calcifications (A). Synthesized S2D mammography image (C-View) with identification of amorphous and segmental calcifications (B). The biopsy confirmed the diagnosis of Ductal Carcinoma in Situ (DCIS)
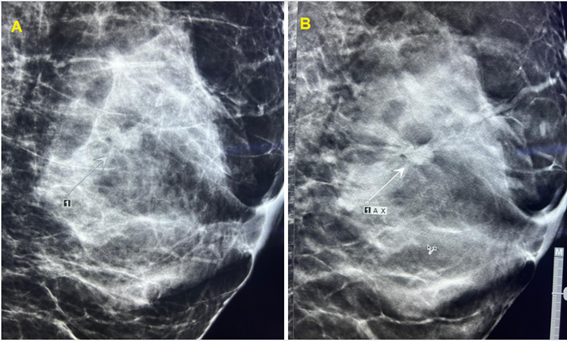
Figure 2. Visualization of a nodule with 2D FFDM mammography (A). Improved definition of the nodule margin on 3D Tomosynthesis – DBT (B)
Finally, the radiation doses emitted by the X-ray tube (Entrance Surface Air Kerma – ESAK), used for each imaging modality, in mediolateral oblique (MLO) and craniocaudal (CC) incidences, were collected from the DICOM files and presented the following results with a 95% confidence interval:
● FFDM – Total radiation dose – ESAK = 9.4±0.6 mGy
● 3D DBT – Total radiation dose – ESAK = 10.3±0.9 mGy
● Combo [FFDM + 3D DBT] – Total radiation dose – ESAK = 19.7±0.4 mGy
DISCUSSION
This study provided important evidence on the comparative performance of FFDM, S2D (C-View), and DBT mammography in the detection and classification of breast lesions, as well as their diagnostic quality in relation to the biopsy gold standard.
The total number of patients (n=149) can be regarded as sufficient for a study validating imaging modalities, particularly in consideration of the richness of data per lesion and the detailed comparative analysis. However, for a more comprehensive understanding of the results, multicenter studies with a larger sample should be performed in the future.
The substantial agreement (Kappa κ=0.757) between FFDM and S2D (C-View) for lesion detection, and even higher for lesion classification (κ=0.867), strongly suggests that S2D has the potential to replace FFDM. This substitution offers significant advantages, including a reduction in the patient's radiation dose, a shorter examination time, less discomfort for patients due to less compression time and fewer exposures.
On the other hand, the lower agreement of DBT with 2D modalities (FFDM and S2D) in lesion detection (κ≈0.22) and the moderate agreement in lesion classification (κ≈0.68) should not be interpreted as an inferior performance of DBT, as they merely indicate that the imaging modalities are different. Indeed, the results of this study demonstrated that DBT exhibited 100% sensitivity in detecting malignant lesions and detected four such lesions not identified by FFDM, thereby indicating its enhanced ability to discern lesions that might otherwise go unnoticed on 2D images. This result validates the hypothesis that DBT facilitates superior visualization of hidden lesions by attenuating the tissue superposition effect, which is a fundamental limitation of 2D images11.
The disparities in sensitivity and accuracy among the modalities confirm this trend. While FFDM and S2D (C-View) demonstrated comparable and high sensitivities and accuracies (above 0.92), yet in this study, DBT exhibited superior performance with 100% sensitivity and 0.964 accuracy. This finding indicates that DBT is a highly effective tool for the detection of malignancies, which is a crucial aspect of early diagnosis. The detection of benign lesions exclusively on FFDM and S2D images (one asymmetry in each modality) can be attributed to the nature of some lesions that sometimes do not show up clearly on layered DBT images4,5.
It is important to emphasize that the market offers different techniques and algorithms for the implementation of tomosynthesis (DBT) and synthesized S2D mammography, in addition to C-View technology12,13. Each company may employ its own algorithms for the reconstruction of the 2D image from DBT images. The quality of the synthesized image, the sensitivity of lesion detection, and also the radiation dose can all be influenced by these different implementations. Various algorithms can differ in terms of factors such as spatial resolution, image contrast, noise suppression, and the false-positive rate. These factors can have an impact on the clinical decision regarding the replacement of FFDM mammography with S2D. Further comparative studies are required among the various implementations of S2D mammography available on the market in order to facilitate an appropriate choice and to encourage the further development of this technology13-15. Although DBT technology offers clear clinical advantages, the high acquisition and maintenance costs must be addressed carefully.
Moreover, it is important to mention some additional technical factors that corroborate the advantages of replacing conventional mammography with synthesized mammography. The reduction in the number of radiation emissions could extend the lifespan of the X-ray tube due to less wear and tear and would allow for a reduction in maintenance costs.
Given the possibility of no longer performing conventional mammography, there is a reduction in breast compression time, which likely provides greater patient comfort. It is important to emphasize that by using the [S2D (C-View) + DBT] combination of imaging modalities instead of the conventional [FFDM + DBT] combination, there will be a significant reduction of about 47.8% in the radiation dose emitted by the X-ray tube and received by the patient. This finding is consistent with results from Zeng et al. and Svahn et al.15,16 that have reported a comparable dose reduction.
Another relevant point to consider is that the interpretation of DBT images is more complex than that of 2D mammograms. The radiologist needs to analyze dozens of images instead of just four 2D images (CC and MLO for each breast). This requires specialized training and a period of adaptation for the professional to become proficient in identifying calcifications, distortions, and other subtle changes. In addition, the large amount of data generated in a single tomosynthesis exam can be challenging for storage and processing in clinics and hospitals. Finally, the analysis of a complete tomosynthesis study also requires more time of the radiologist5.
This study was performed with a Selenia Dimensions (Hologic) mammography machine, installed in 2017 at INCA's Breast Radiology Service (SEDIM-HC3). Recently, a new Selenia 3D Dimensions Hologic device was incorporated into SEDIM-HC3, featuring new functionalities and more advanced technologies, such as a new high-resolution image receptor (High Resolution – HR of 70 micrometers)17 and intelligent reconstruction software, which allows for better quality images, with greater speed and easier to read. This equipment also has more efficient workstations and video monitors, enabling faster and more accurate diagnoses, as well as better image resolution. This scenario allows for new research to be carried out at INCA in the near future. Another area of interest for future studies at the institution is the use of deep learning techniques on radiology images to improve breast cancer diagnosis.
This study has some limitations. Data were collected in 2019, and therefore do not fully capture the most recent technological advances available in 2025. Furthermore, the fact that it is a single-center study with symptomatic patients or patients with previous abnormal findings on imaging tests may limit the generalizability of the results. Nevertheless, the findings remain clinically relevant as they provide robust evidence supporting S2D as a substitute for FFDM and establish a benchmark for future comparisons with newer systems. Future research should focus on multicenter validation with larger cohorts including asymptomatic patients or patients without previous abnormal findings on imaging tests, integration of high-resolution detectors, and the use of artificial intelligence and deep learning tools to optimize lesion detection.
CONCLUSION
In this study, synthesized S2D mammography (C-View) confirmed its potential to replace traditional Full-Field Digital Mammography (FFDM), offering benefits such as a reduced radiation dose and least patient discomfort, without compromising diagnostic accuracy. The results demonstrated excellent statistical agreement (Kappa index greater than 0.75) with conventional FFDM for both lesion detection and classification.
On the other hand, tomosynthesis (DBT) showed a superior ability to detect malignant lesions (100% sensitivity), including those not visible on 2D images, reinforcing its value as an appropriate and necessary imaging modality for breast cancer diagnosis.
In conclusion, it is clear that in the INCA setting, the combination of DBT with S2D (C-View) functions as an appropriate and optimized alternative, allowing for a reduced radiation dose, in addition to more accurate breast cancer screening and diagnosis for the Brazilian population.
CONTRIBUTIONS
Paula Medina Maciel Gomes Curi Bonotto contributed to the conception and design of the study, acquisition, analysis, and interpretation of the data and critical review. Léonie Marie Catherine Lefebvre and Carlos Frederico Motta Vasconcelos contributed to the acquisition, analysis, and interpretation of the data, writing and critical review. Antonio Mauricio Ferreira Leite Miranda de Sá contributed to the interpretation of the data, and critical review. Anke Bergmann and Suzana Sales de Aguiar contributed to the conception and design of the study, and critical review. All the authors approved the final version for publication.
STATEMENT OF CONFLICT OF INTEREST
The author Anke Bergmann declares a potential conflict of interest because she is the scientific-editor of INCA’s Revista Brasileira de Cancerologia. The other authors do not have any conflicts of interest.
STATEMENT OF DATA AVAILABILITY
The data should be requested to the corresponding author by e-mail.
FUNDING SOURCES
None.
REFERENCES
1. World Health Organization [Internet]. Geneva: WHO; 2025. Breast cancer, 2025 Aug 14 [cited 2025 set 12]. Available from: https://www.who.int/news-room/fact-sheets/detail/breast-cancer
2. Instituto Nacional de Câncer [Internet]. Rio de Janeiro: INCA; 2023. Outubro Rosa 2022, 2023 Mar 29 [cited 2025 jul 13]. Available from: https://www.gov.br/inca/pt-br/assuntos/campanhas/2022/outubro-rosa
3. Instituto Nacional de Câncer. Controle do câncer de mama no Brasil: dados e números [Internet]. Rio de Janeiro: INCA; 2024 [cited 2025 jul 13]. Available from: https://www.inca.gov.br/publicacoes/livros/controle-do-cancer-de-mama-no-brasil-dados-e-numeros-2024
4. García AMR, Fernández DM. Breast tomosynthesis: state of the art. Radiología. 2019;61(4):274-85. doi: https://doi.org/10.1016/j.rx.2019.01.002
5. Kleinknecht JH, Ciurea AI, Ciortea CA. Pros and cons for breast cancer screening with tomosynthesis a review of the literature. Med Pharm Rep. 2020;93(4):335-41. doi: https://doi.org/10.15386/mpr-1698
6. Xu H, Xu B. Breast cancer: epidemiology, risk factors and screening. Chin J Cancer Res. 2023;35(6):565-83. doi: https://doi.org/10.21147/j.issn.1000-9604.2023.06.02
7. Hologic [Internet]. C-View Synthesised 2D Imaging. [date unknowndate]: Hologic; ©2025 [cited 2025 jul]. Available from: https://www.hologic.co.uk/en-gb/products/c-view-synthesised-2d-imaging#4257225834-665754410
8. US Food and Drug Administration. Premarket Approval (PMA) [Internet]. Silver Spring: USFood Drug Administration; 2025 [cited 2025 jul 12]. Available from: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpma/pma.cfm?id=P080003S001
9. Fleiss JL. Statistical methods for rates and proportions. 2ed. New York: John Wiley & Sons; 1981.
10. Conselho Nacional de Saúde (BR). Resolução n° 466, de 12 de dezembro de 2012. Aprova as diretrizes e normas regulamentadoras de pesquisas envolvendo seres humanos [Internet]. Diário Oficial da União, Brasília, DF. 2013 jun 13 [cited 2025 ago 27]; Seção 1:59. Available from: https://bvsms.saude.gov.br/bvs/saudelegis/cns/2013/res0466_12_12_2012.html
11. Hamad W, Michell MJ, Myles JP, et al. Diagnostic performance of tomosynthesis plus synthetic mammography versus full-field digital mammography with or without tomosynthesis in breast cancer screening: a systematic review and meta-analysis. Int J Cancer. 2025;156(5):969-79. doi: https://doi.org/10.1002/ijc.35217
12. Rodriguez-Ruiz A, Teuwen J, Vreemann S, et al. New reconstruction algorithm for digital breast tomosynthesis: better image quality for humans and computers. Acta Radiol. 2018;59(9):1051-9. doi: https://doi.org/10.1177/0284185117748487
13. Heywang-Köbrunner SH, Jänsch A, Hacker A, et al. Digital breast tomosynthesis (DBT) plus synthesised two-dimensional mammography (S2D) in breast cancer screening is associated with higher cancer detection and lower recalls compared to digital mammography (DM) alone: results of a systematic review and meta-analysis. Eur Radiol. 2022;32:2301-12. doi: https://doi.org/10.1007/s00330-021-08308-8
14. Heywang-Köbrunner SH, Jänsch A, Hacker A, et al. Tomosynthesis with synthesised two-dimensional mammography yields higher cancer detection compared to digital mammography alone, also in dense breasts and in younger women: a systematic review and meta-analysis. Eur J Radiol. 2022;152:110324. doi: https://doi.org/10.1016/j.ejrad.2022.110324
15. Zeng B, Yu K, Gao L, et al. Breast cancer screening using synthesized two-dimensional mammography: a systematic review and meta-analysis. Breast. 2021;59:270-8. doi: https://doi.org/10.1016/j.breast.2021.07.016
16. Svahn TM, Houssami N, Sechopoulos I, et al. Review of radiation dose estimates in digital breast tomosynthesis relative to those in two-view full-field digital mammography. Breast. 2015;24(2):93-9. doi: https://doi.org/10.1016/j.breast.2014.12.002
17. Talley M, Starzyk K, Pohlman S, et al. Mammography screening outcomes for women screened by standard versus high resolution digital breast tomosynthesis. Clin Imaging. 2025;125:110553. doi: https://doi.org/10.1016/j.clinimag.2025.110553
Recebido em 9/9/2025
Aprovado em 10/11/2025
Executive-editor: Letícia Casado. Orcid iD: https://orcid.org/0000-0001-5962-8765
![]()
Este é um artigo publicado em acesso aberto (Open Access) sob a licença Creative Commons Attribution, que permite uso, distribuição e reprodução em qualquer meio, sem restrições, desde que o trabalho original seja corretamente citado.