Artificial Intelligence in Cancer Control: A Global Bibliometric Analysis of Trends, Applications, and Implementation Challenges
Inteligência Artificial no Controle do Câncer: Uma Análise Bibliométrica Global de Tendências, Aplicações e Desafios de Implementação
Inteligencia Artificial en el Control del Cáncer: Un Análisis Bibliométrico Global de Tendencias, Aplicaciones y Desafíos de Implementación
https://doi.org/10.32635/2176-9745.RBC.2026v72n2.5614
Martins Fideles dos Santos Neto1; Carina Munhoz de Lima2; Camila Belo Tavares Ferreira3; Robson Dias Martins4; Moreno Muniz Euzébio Rodrigues da Silva5; Kesya Cristina Silva de Paula6; Telma de Almeida Souza7; Paulo Roberto de Jesus Dantas8; Ricardo Vela de Britto Pereira9; Alessandra de Sá Earp Siqueira10
1,3-8,10Instituto Nacional de Câncer (INCA), Coordenação de Ensino (Coens). Rio de Janeiro (RJ), Brasil. E-mails: martins_neto17@hotmail.com; camila.ferreira@inca.gov.br; robson.martins@inca.gov.br; moreno.silva@ensino.inca.gov.br; kesya.paula@inca.gov.br; tsouza@inca.gov.br; paulo.dantas@inca.gov.br; asiqueira@inca.gov.br. Orcid iD: https://orcid.org/0000-0003-2996-2222; Orcid iD: https://orcid.org/0000-0002-1423-513X; Orcid iD: https://orcid.org/0000-0002-5825-9408; Orcid iD: https://orcid.org/0009-0008-6738-018X; Orcid iD: https://orcid.org/0000-0001-7342-1971; Orcid iD: https://orcid.org/0000-0003-2786-1890; Orcid iD: https://orcid.org/0009-0007-6606-097X; Orcid iD: https://orcid.org/0000-0003-3852-7580
2INCA, Coens, Revista Brasileira de Cancerologia (RBC). Rio de Janeiro (RJ), Brasil. Universidade Federal Fluminense (UFF), Pós-Graduação em Ciência da Informação (PPGCI). Niterói (RJ), Brasil. E-mail: carina.lima@inca.gov.br. Orcid iD: https://orcid.org/0000-0002-1615-9177
9Universidade Estadual do Rio de Janeiro (Uerj), Instituto de Matemática e Estatística (IME). Rio de Janeiro (RJ), Brasil. E-mail: ricardo.vela@uerj.br. Orcid iD: https://orcid.org/0000-0003-1473-2889
Corresponding author: Martins Fideles dos Santos Neto. Rua Marques de Pombal, 125 – Centro. Rio de Janeiro (RJ), Brasil. CEP 20230-240. E-mail: martins_neto17@hotmail.com
ABSTRACT
Introduction: Artificial intelligence (AI) has been increasingly applied across the cancer control continuum, encompassing prevention, early detection, diagnosis, treatment, and health system management. The rapid growth of AI research in oncology reflects methodological diversity and global interest, with variability in implementation and validation contexts. Objective: To map the global scientific output on AI applications in cancer prevention and control, identifying publication trends, geographic distribution, study designs, types of AI, levels of implementation, and implications for health systems and public policies. Method: A bibliometric review following Donthu et al. Searches were conducted in six databases in April 2025, guided by PRISMA principles. Screening and eligibility were independently performed by two reviewers, with a third reviewer for adjudication. Variables: year, authorship/affiliation, journals, countries, keywords, study design, cancer type, control phase, AI type, level of implementation, cost-effectiveness, and Big Data. Analyses were conducted using Excel, VOSviewer, and EndNote. Results: Of 482 records, 134 studies were included. Publications increased after 2021, particularly in high-income countries (United States and China). Machine learning and deep learning predominated. Approximately one-third reported real-world clinical application; most studies were observational, narrative, or modeling-based. Few addressed cost-effectiveness or large-scale Big Data. Conclusion: There is sustained growth and diversification of AI in cancer control, with emphasis on diagnosis and treatment, heterogeneous levels of implementation, and relevance for health system organization and policy, including in low-resource settings.
Key words: Artificial Intelligence; Bibliometrics; Big Data; Scientific Publication Indicators; Science, Technology and Society.
RESUMO
Introdução: A inteligência artificial (IA) tem sido cada vez mais aplicada ao longo do continuum de controle do câncer, abrangendo prevenção, detecção precoce, diagnóstico, tratamento e gestão dos sistemas de saúde. O rápido crescimento da pesquisa em IA em oncologia reflete diversidade metodológica e interesse global, com variabilidade nos contextos de implementação e validação. Objetivo: Mapear a produção científica global sobre aplicações de IA na prevenção e no controle do câncer, identificando tendências de publicação, distribuição geográfica, desenhos de estudo, tipos de IA, níveis de implementação e implicações para sistemas de saúde e políticas públicas. Método: Revisão bibliométrica conforme Donthu et al. Buscas em seis bases de dados em abril de 2025, guiadas por princípios PRISMA. Triagem e elegibilidade por dois revisores de forma independente, com terceiro para adjudicação. Variáveis: ano, autoria/afiliação, periódicos, países, palavras-chave, desenho, tipo de câncer, fase do controle, tipo de IA, nível de implementação, custo-efetividade e Big Data. Análise com Excel, VOSviewer e EndNote. Resultados: De 482 registros, 134 estudos foram incluídos. As publicações aumentaram após 2021, sobretudo em países de alta renda (EUA e China). Predominaram machine learning e deep learning. Cerca de um terço relatou aplicação clínica no mundo real; a maioria foi observacional, narrativa ou de modelagem. Poucos abordaram custo-efetividade ou Big Data em larga escala. Conclusão: Há crescimento e diversificação sustentados da IA no controle do câncer, com ênfase em diagnóstico e tratamento, níveis heterogêneos de implementação e relevância para organização do sistema e políticas, inclusive em contextos com poucos recursos.
Palavras-chave: Inteligência Artificial; Bibliometria; Big Data; Indicadores de Produção Científica; Ciência, Tecnologia e Sociedade.
RESUMEN
Introducción La inteligencia artificial (IA) se ha aplicado cada vez más a lo largo de la continuidad del control del cáncer, abarcando la prevención, la detección temprana, el diagnóstico, el tratamiento y la gestión de los sistemas de salud. El rápido crecimiento de la investigación en IA en oncología refleja diversidad metodológica e interés global, con variabilidad en los contextos de implementación y validación. Objetivo: Mapear la producción científica global sobre las aplicaciones de la IA en la prevención y el control del cáncer, identificando tendencias de publicación, distribución geográfica, diseños de estudio, tipos de IA, niveles de implementación e implicaciones para los sistemas de salud y las políticas públicas. Método: Revisión bibliométrica conforme con Donthu et al. Se realizaron búsquedas en seis bases de datos en abril de 2025, guiadas por los principios PRISMA. La selección y elegibilidad fueron realizadas de forma independiente por dos revisores, con un tercero para la adjudicación. Las variables fueron año, autoría/afiliación, revistas, países, palabras clave, diseño del estudio, tipo de cáncer, fase del control, tipo de IA, nivel de implementación, coste-efectividad y Big Data. El análisis se llevó a cabo con Excel, VOSviewer y EndNote. Resultados: De 482 registros, se incluyeron 134 estudios. Las publicaciones aumentaron después de 2021, especialmente en países de altos ingresos (Estados Unidos y China). Predominaron el machine learning y el deep learning. Aproximadamente un tercio informó aplicaciones clínicas en el mundo real; la mayoría fueron estudios observacionales, narrativos o de modelado. Pocos abordaron la relación coste-efectividad o el Big Data a gran escala. Conclusión: Existe un crecimiento y una diversificación sostenidos de la IA en el control del cáncer, con énfasis en el diagnóstico y el tratamiento, niveles heterogéneos de implementación y relevancia para la organización del sistema y las políticas, incluso en contextos con recursos limitados.
Palabras clave: Inteligencia Artificial; Bibliometría; Big Data; Indicadores de Producción Científica; Ciencia, Tecnología y Sociedad.
INTRODUCTION
Artificial Intelligence (AI) is increasingly reshaping cancer care, offering novel capabilities for early detection1, risk stratification2, treatment guidance3, and health system optimization4,5. Machine learning (ML) and deep learning (DL) models have demonstrated promising results in interpreting complex clinical, genomic, and imaging data, supporting personalized decision-making in oncology6-9. For example, AI-enhanced screening tools in colorectal cancer have shown improvements in polyp detection accuracy, reducing human error and improving diagnostic yield10. Moreover, integration with robotic surgery, computer-aided detection (CADe), and large-scale clinical data is enabling more precise, real-time cancer management10. These tools not only augment clinicians’ capabilities but also present opportunities for decentralizing specialized oncology services, particularly in resource-limited settings.
Despite these advantages, the implementation of AI in cancer control presents notable limitations and challenges. A significant proportion of published models remain in experimental or proof-of-concept phases, lacking robust external validation or clinical integration11-13. Issues such as limited generalizability, algorithmic opacity, lack of standardized datasets, and risks of automation bias hinder safe translation into practice. Ethical and regulatory concerns also persist, including data privacy, consent, accountability for AI-driven decisions, and potential inequities in access to AI-based interventions14,15. Furthermore, while AI systems are often trained on data from high-income regions, their deployment in low- and middle-income countries (LMICs) where they may have the greatest potential requires socio-contextual adaptation and infrastructural support16-18.
Given the potential of AI to advance cancer control while also introducing new challenges, a comprehensive bibliometric review is needed. This study aims to map global scientific production on AI in oncology, identifying trends, implementation levels, types of AI used, and their relevance to cancer control policies in both high-income and resource-constrained countries.
METHOD
The present study is a bibliometric analysis and a literature review. This investigation was structured according to the framework outlined by Donthu et al.¹⁹, and the bibliometric analysis was conducted through a four-phase process.
Step 1: define the aims and scope of the bibliometric study
This bibliometric review aims to map the scientific landscape and thematic trends in the application of AI for cancer prevention and control. Guided by the overarching research question, “Is AI a solution or a challenge in the oncological field?”, this study explores a set of specific inquiries: (1) Which types of AI are most frequently employed in oncology-related research? (2) What cancer specialties are most commonly addressed in these AI applications? (3) How are themes such as big data and cost-effectiveness discussed in the literature? (4) What are the dominant journals, countries, and authors contributing to this field? and (5) What keyword patterns and co-authorship networks characterize this body of research? By addressing these questions, this review not only provides a comprehensive overview of existing studies but also highlights emerging directions and thematic concentrations, fulfilling the core purpose of a bibliometric analysis: to reveal intellectual structures and guide future research agendas.
Step 2: choose the techniques for bibliometric analysis
Initially, the study selection process was systematically guided by the PRISMA20 (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) (Figure 1) flow diagram, which documented each phase of data screening and inclusion. An Excel spreadsheet was then developed to organize both morphological variables (such as article title, authorship, year of publication, scientific journal, and country of origin) and thematic variables (including the type of used, its primary objective, cancer control phase targeted, level of implementation, and cost-effectiveness). All data were manually extracted from the eligible articles and systematically input into the spreadsheet for further analysis.
Quantitative metrics related to authorship were retrieved using the Scopus database, which provided information on h-index, total number of documents published, citation counts, and institutional affiliations. For network visualization and relationship mapping, the VOSviewer software was employed. This tool enabled the construction of co-authorship networks (Figure 2A), heat maps (Figure 1 of the supplementary material 1), and co-occurrence analyses of keywords (Figure 2B) revealing the intellectual structure and thematic focus of the field. The quantitative analysis relied on frequency and percentage calculations with Microsoft Excel used for data tabulation and processing.
To enhance geographic interpretation, a spatial representation of contributing countries was developed using Canva (an online graphic design platform that allows users to create visual materials), with a focus on nations with the highest publication counts. Descriptive analyses addressing broader themes, such as the role of AI in cancer control for public health policies in low- and middle-income countries like Brazil, were carried out through interpretive readings and synthesis by the research team.
Step 3: collect the data for bibliometric analysis
The literature search for this bibliometric study was conducted across six major databases: PubMed, EMBASE, Scopus, BVS, LILACS, and Web of Science (WOS). A specialized health sciences librarian developed the search strategy (Supplementary Material 2), combining the descriptors "Artificial Intelligence," "Cancer," and "Prevention and Control." For this research topic, the search strategy was deliberately limited to title-based retrieval, based on pilot tests comparing title-only versus title-and-abstract screening. Expanding to abstracts markedly reduced specificity, generating many irrelevant records and conceptual noise without a meaningful gain in sensitivity. In AI applied to cancer control, studies that truly address both core dimensions typically state them explicitly in the title, consistent with field norms. Thus, title restriction improved precision while maintaining comprehensiveness, though this approach is not broadly generalizable to other topics.
Study selection was conducted independently in duplicate by two reviewers, assessing titles/abstracts and full texts against predefined eligibility criteria. Disagreements were resolved by discussion, and a third reviewer, an expert in cancer prevention, adjudicated unresolved cases until consensus was reached. Searches were performed in April 2025, and included studies published up to that date, establishing a clear temporal cutoff for analysis and future updates. Eligibility criteria included studies that explicitly addressed the relationship between AI and cancer within a preventive or control framework. In this context, cancer control encompasses not only early detection and primary prevention but also treatment and long-term management strategies, recognizing the conceptual integration of therapeutic and prognostic interventions. No time limits were applied, but duplicates and records not primarily focused on the AI–cancer relationship were excluded. Only studies in English, Portuguese, or Spanish were included. Data were managed and organized using EndNote X9.
Step 4: run the bibliometric analysis and report the findings
This bibliometric review provides a clear and structured synthesis of scientific production on the use of AI in cancer control. It follows standard bibliometric procedures, including PRISMA flowchart tracking and keyword co-occurrence mapping with VOSviewer.
RESULTS
A total of 482 records, obtained from the combined results of all selected databases, were initially screened, from which 134 studies were deemed eligible for inclusion in this bibliometric review.
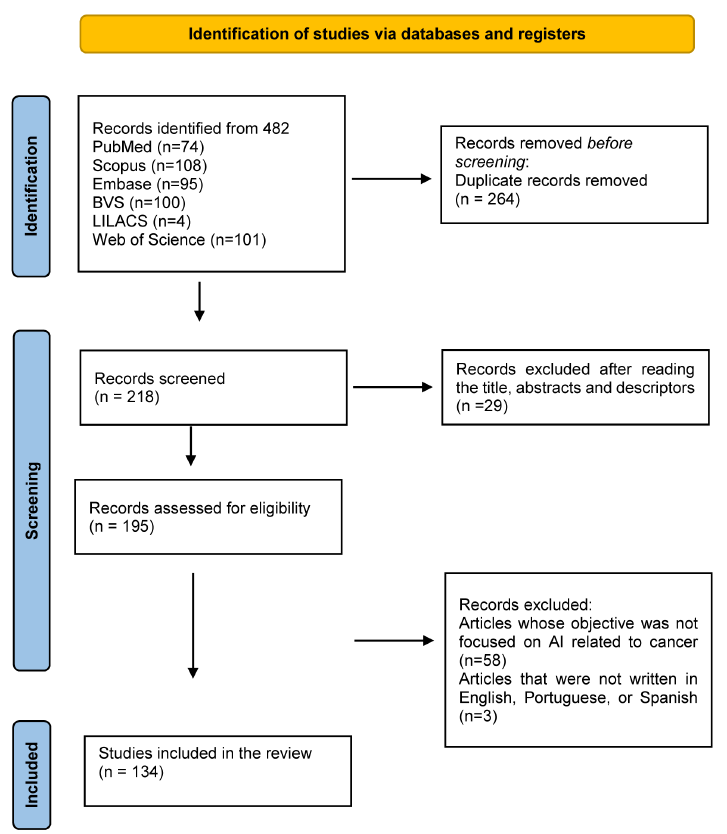
Figure 1. PRISMA flowchart for article selection in the databases
Source: Adapted from PRISMA 202020.
Year
Among the 134 articles analysed, the majority were published in recent years, reflecting the accelerating interest in applying AI to cancer control. The year 2024 accounted for the highest number of publications, with 44 articles (32.8%), followed by 2023 with 27 articles (20.1%), and 2025 with 25 articles (18.7%). This upward trend began in 2021, with 9 articles (6.7%), and continued through 2022, which saw 17 publications (12.7%). In earlier years, the volume was significantly lower: 2015 had only 2 articles (1.5%), 2016 and 2018 had 1 article each (0.7%), 2019 had 3 articles (2.2%), and 2020 had 5 articles (3.7%).
Author
In the bibliometric analysis conducted using VOSviewer software, a total of 833 unique authors were identified across the 134 eligible articles. Of these, only 28 authors were found to have established co-authorship links with one another, indicating formal collaborations reflected in joint publications. In VOSviewer, such connections referred to as “links” represent shared authorship on at least one publication, suggesting scholarly cooperation and potential intellectual exchange between the researchers involved. The relatively low number of co-authorship links highlights a fragmented research landscape with limited collaboration among contributors. The five authors with the highest number of co-authorship links are detailed in Table 1. The heatmap presents the five authors (Figure 1 of the supplementary material 1).
Table 1. Five authors with the highest number of co-authorship
|
Author |
Documents |
Citations |
h-index |
Co-authors |
Affiliation |
|
|
Cesare Hassan |
887 |
38,432 |
96 |
3,141 |
Humanitas University. The institution will open in a new tab, Pieve Emanuele, Italy |
|
|
Alessandro Repici |
796 |
27,319 |
81 |
3,146 |
Humanitas University. The institution will open in a new tab, Pieve Emanuele, Italy |
|
|
Miguel Areia |
74 |
3,869 |
25 |
656 |
Portuguese Oncology Institute of Coimbra, Coimbra, Portugal |
|
|
Giulio Antonelli |
101 |
3,983 |
30 |
776 |
Sapienza Università di Roma. The institution will open in a new tab, Rome, Italy |
|
|
Marco Spadaccini |
145 |
4,424 |
33 |
638 |
Humanitas Research Hospital. The institution will open in a new tab, Rozzano, Italy |
Affiliations
The institutional landscape of authorship is notably diverse, reflecting both the global interest and multidisciplinary nature of AI applications in cancer control. A substantial proportion of studies originate from academic medical centers and research hospitals in China (with over 25 institutions, approximately 36.2%), with recurring institutions such as Shanghai Jiao Tong University, Fudan University, Zhejiang University, and the Chinese Academy of Sciences, underscoring the country’s significant investment in oncology research and AI integration. The United States (15 institutions, 21.7%) also figures prominently, particularly with contributions from Stanford University, MD Anderson Cancer Center, Harvard Medical School, and Memorial Sloan Kettering Cancer Center, often in collaborative networks that span multiple states or countries. European (cumulatively accounting for 17 institutions, 24.6%) representation is robust, with institutions such as Heidelberg University, Karolinska Institutet, University College London, University of Padova, and Humanitas University contributing to large-scale, often multicentric studies. In the Global South, key contributions were observed from Brazil (Universidade Positivo), India (PGIMER, Amrita Institute), Pakistan, Bangladesh, and South Africa (University of Pretoria), often focusing on the adaptation of AI tools to local health system contexts. Additionally, LLM (Large Language Model)-based models such as ChatGPT and OncoGPT were frequently authored in collaborative studies involving institutions from Canada, Israel, South Korea, and Australia (figure 2c).
Keyword
The analysis of the keyword descriptors across the included studies reveals dominant trends and emerging themes in the field of AI applied to cancer care. The term "artificial intelligence" appeared most frequently, cited in 12 instances (11.43%), affirming its central role in the thematic scope of the reviewed literature. Other prevalent keywords included "deep learning" (6 occurrences, 5.71%), "machine learning" (5, 4.76%), and "hepatocellular carcinoma" (3, 2.86%), indicating a significant focus on technical methodologies and liver-related oncology. Additional keywords such as "cancer treatment," "personalized medicine," "cancer," "ChatGPT," "lung cancer," "radiomics," "diagnosis," "treatment," "precision medicine," and "breast cancer" each appeared in 2 occurrences (1.90%), reflecting broader interests in oncology subtypes, diagnostic processes, and therapy personalization. In contrast, descriptors like "generative AI chatbot," "intermittent androgen deprivation therapy," and "large language model" were among the least mentioned, each appearing only once, suggesting that these remain emerging or niche topics within the field.
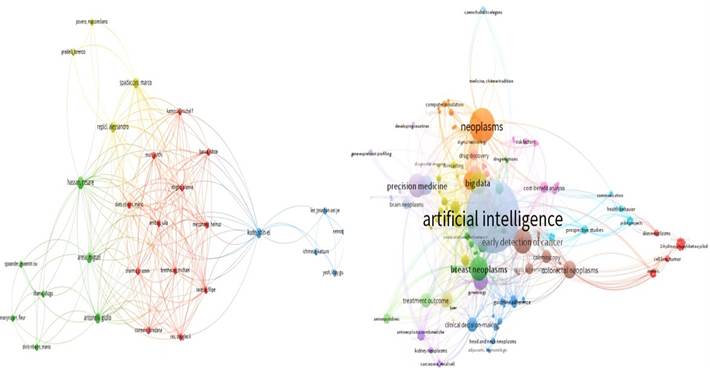
Figure 2. A The co-authorship links and B Analysis of Descriptors and Keyword Frequencies
Journals
The most frequent journal was Cureus, with 5 occurrences (3.7%), followed by Frontiers in Oncology and Current Oncology, each appearing 4 times (3.0%). Diagnostics, European Journal of Cancer, Seminars in Cancer Biology, and Revista Brasileira de Cancerologia each appeared 3 times (2.2%). Additionally, Scientific Reports, European Journal of Radiology, Frontiers in Digital Health, Journal of Clinical Medicine, NPJ Precision Oncology, Cancer Discovery, and Biomedical Signal Processing and Control were each cited twice (1.5%). The remaining 112 journals (83.6%) appeared only once, indicating a broad dispersion of publication sources across disciplines such as oncology, digital health, radiology, and molecular sciences. This diversity underscores the interdisciplinary nature of research on AI in cancer prevention and control.
Country
Although the review includes 134 eligible articles, several studies were multicentric, resulting in a total of 212 country occurrences. The United States was the most frequently represented, appearing 40 times (18.9%), followed by China with 34 occurrences (16%), and Germany with 14 occurrences (6.6%). The highlighted countries had the highest number of publications in the sample. Countries with at least 2 occurrences (0.9%) are displayed in the image (Figure 3).

Figure 3. Countries occurrences
Study Design
Narrative reviews were the most prevalent, with 65 occurrences (48.5%), followed by predictive modeling studies, including both theoretical and experimental approaches, totaling 31 studies (23.1%). Observational studies both prospective and retrospective accounted for 26 instances (19.4%), while systematic reviews appeared in 7 studies (5.2%). Experimental studies and pilot trials, including in vitro and in vivo validations or clinical simulations, represented 9 cases (6.7%).
Population Sample
Among the 134 eligible studies, only 41 studies (30.6%) included real patient data. The cumulative number of patients across these studies totaled approximately 352,274 individuals. The most represented cancer types were breast cancer, with over 71,000 patients (20.2%), colorectal cancer, including colon and rectal subtypes, with over 81,000 patients (23.0%), and hepatocellular carcinoma, with 4,486 patients (1.3%). Lung cancer appeared in various studies, contributing with approximately 6,000 patients (1.7%). Additionally, studies involving mixed cancer populations or broader oncological cohorts accounted for over 177,000 patients with oral cancer (50.2%), largely derived from large national registries or simulation models. The remaining patients were distributed across studies involving cervical, prostate, renal, and pediatric cancers. Notably, the majority of included articles were reviews or theoretical studies without direct empirical samples, emphasizing a reliance on secondary data or simulation rather than original patient-based research.
Healthcare professional specialty
Oncology was the most prevalent specialty, present in 100% of the studies (134/134), followed by radiology in approximately 86 studies (64.2%), and pathology, which appeared in 78 studies (58.2%). Surgical oncology, radiotherapy, and bioinformatics were also highly represented, each featured in over 40 studies (29.9%). Other frequently involved specialties included public health (≈35%), genetics/genomics (≈25%), gastroenterology, urology, gynecology, and dermatology, depending on the cancer type and AI application. The presence of engineering, informatics, molecular biology, and nursing underscores the growing integration of computational, translational, and clinical fields.
Types of Cancer
Colorectal cancer was the most frequently mentioned, appearing in 27 studies (20.1%), followed closely by breast cancer cited in 25 studies (18.7%). Lung cancer was also highly represented, featured in 23 studies (17.2%), particularly non-small cell lung cancer (NSCLC). Other common focuses included hepatocellular carcinoma (HCC) in 9 studies (6.7%), and prostate cancer, in 8 studies (6.0%). Several articles addressed multiple cancer types simultaneously, often integrating AI tools across various tumor entities (e.g., breast, lung, colorectal, prostate, and brain cancers), totaling 42 studies (31.3%). Less common, yet specifically targeted, were cancers such as cervical, gastric, oral, and gliomas.
Aspects of cancer control
Among the 134 analyzed articles, 81 studies (60.4%) addressed both prevention and treatment dimensions of cancer control, reflecting an integrated approach to early detection, diagnosis, and therapeutic management. 48 studies (35.8%) focused exclusively on treatment, including interventions such as chemotherapy response, surgical planning, and supportive care. Only 5 studies (3.7%) were dedicated solely to prevention, primarily targeting early detection, screening, and risk reduction strategies. These findings indicate a strong predominance of treatment-oriented research, while also highlighting a growing emphasis on combined strategies that align with the continuum of cancer care. In another perspective, 97 studies (72.4%) explicitly addressed tertiary prevention, focusing on controlling disease progression, managing treatment response, avoiding complications, and improving quality of life after cancer diagnosis. Additionally, 33 studies (24.6%) combined secondary and tertiary prevention, integrating early detection strategies such as screening and diagnostic stratification—with therapeutic interventions and prognostic monitoring.
Artificial Intelligence as a Solution in Cancer Control
AI was mainly presented as a tool for cancer control, with over 90% of studies linking it to better early detection, diagnostic accuracy, treatment personalization, and clinical decision support. Applications spanned screening/triage, treatment planning and response prediction, and supportive care (e.g., psychological and nutritional). In radiology and pathology, AI automated image analysis, reduced interobserver variability, and supported timely interventions. It also enabled risk stratification, biomarker discovery, and drug development for precision oncology. Despite noted ethical issues, technical limits, and the need for clinical validation, the overall literature portrays AI as transformative across the cancer care continuum.
Barriers to Artificial Intelligence in Cancer Control
Despite its vast potential, the implementation of AI in cancer control faces several critical barriers. Chief among these is the need to reduce clinical variability in therapeutic decisions and promote evidence-based, personalized treatment recommendations, a challenge driven by the complexity and heterogeneity of cancer presentations. AI seeks to address persistent issues such as delayed diagnosis, low detection rates in early stages, limited access to specialists, and the inefficiency of manual data interpretation, especially in radiology, pathology, and genomics. In resource-constrained settings, AI could mitigate the shortage of trained personnel and improve adherence to clinical guidelines. However, barriers to widespread adoption include ethical concerns, lack of validation in real-world clinical settings, data fragmentation, and limited interpretability of black-box models. Furthermore, the cost, infrastructure requirements, and inequities in data quality and representation pose significant limitations. Ultimately, while AI is positioned to transform cancer care by enabling predictive, preventive, and personalized interventions, its effective integration depends on overcoming technical, regulatory, and systemic challenges.
Level of Implementation of Artificial Intelligence
The level of AI implementation in oncology varied widely. 41 studies (30.6%) reported real-world clinical application, indicating that AI tools were already being used in hospital settings, either in diagnostic support, treatment planning, or patient monitoring. 59 studies (44.0%) were in prototyping or validation phases, including retrospective analyses, simulation environments, or early-stage pilot trials showing significant development, but limited integration into routine clinical care. Additional 34 studies (25.4%) were primarily theoretical or exploratory, focusing on conceptual frameworks, simulation modeling, or proposals for future clinical integration.
Cost-Effectiveness
Among the 134 studies analyzed, the majority did not include formal cost-effectiveness analyses or failed to present concrete economic data, instead offering only conceptual discussions on AI’s potential to reduce costs through automation, early diagnosis, and avoidance of ineffective treatments. However, 12 studies (9.0%) provided quantifiable economic outcomes, supporting AI as a cost-effective strategy in cancer control. For instance, one study reported an incremental cost-effectiveness ratio (ICER) of $8,790/Quality-Adjusted Life Year (QALY) for AI-assisted screening every five years, while another projected an annual saving of $290 million in the U.S. with increased screening adherence. In population-based programs, AI was shown to be dominant (more effective and less costly), improving early detection while reducing overall healthcare expenditure. Specific interventions also demonstrated cost-saving thresholds, such as being cost-effective if AI implementation remained below €100 per patient, or achieving €0.013 per person reached in digital campaigns.
Aspects Related to Big Data
Among the articles reviewed, 89 studies (66.4%) incorporated the concept of Big Data in a substantive way, employing it to train, validate, and optimize AI models for cancer control. These studies utilized large-scale datasets encompassing clinical records, medical imaging (such as radiomics and histopathology), genomics, transcriptomics, and even population-level data from repositories like Surveillance, Epidemiology and End Results (SEER), The Cancer Genome Atlas Program (TCGA), Gene Expression Omnibus (GEO), and chemical database with structures, information and links (PubChem). Common applications included DL for predictive modeling, integration of multimodal data (e.g., imaging and omics), and real-time decision support systems. A subset of these studies also emphasized the importance of data harmonization, interoperability, and reduction of dimensionality, showcasing the increasing technical sophistication in handling large and heterogeneous datasets. Conversely, 45 studies (33.6%) either lacked explicit engagement with Big Data or mentioned it only conceptually, without employing large datasets or advanced data analytics. Most studies relied on small samples, conceptual frameworks, or simulations rather than large-scale data. Many AI tools were trained on narrow datasets or limited to text/language tasks, reducing scalability and generalizability. Overall, the literature shows uneven maturity in data use, and only some studies fully leverage Big Data to improve prediction, personalization, and efficiency in oncology.
Artificial Intelligence in Cancer Control for Public Health Policies in Developing or Underdeveloped Countries, such as Brazil
The reviewed article highlights AI’s strategic value in expanding equitable access to early cancer detection, treatment planning, and follow-up care within Brazil’s National Health System (SUS), especially in underserved areas with a shortage of specialists. Using examples such as AI-assisted triage, radiomics, personalized therapy decision-making, and optimized clinical workflows, it argues that AI tools can reduce delays in care, avoid unnecessary procedures, and lower costs in budget-constrained public systems. It also calls for integrated data infrastructures, national imaging repositories, and regulatory frameworks to ensure safe, ethical, and fair adoption. Finally, it points to scalable, low-cost solutions (e.g., non-invasive screening and AI chatbots) that support health education, risk stratification, and prevention, guiding investment in digital health, workforce training, and evidence-based protocols.
Type of Artificial Intelligence Employed
The 134 AI models analyzed were categorized into five major types. Most studies (96; 73.9%) employed ML and DL approaches, including convolutional neural networks (CNN), radiomics, support vector machines (SVM), and autoencoders. (Figure 2 of the supplementary material 1)
These were broadly applied to colorectal, breast, lung, prostate, liver, gastric, head and neck, brain tumors, and hematological malignancies. Multiple studies within this category also covered pan-cancer models, pediatric oncology, and rare tumor types, reflecting the generalizability and scalability of ML/DL across cancer types. A second group consisted of LLMs and natural language processing (NLP) systems (19; 14.2%), including ChatGPT, OncoGPT, and other transformer-based models. These were primarily applied to breast, colorectal, prostate, and lung cancer, as well as to support education, communication, and triage in oncology care. The third category was Watson for Oncology, an IBM cognitive computing system (5; 3.7%), mainly applied to colorectal, lung, bladder, and hematologic cancers for clinical decision support. The Computer-Aided Detection/Diagnosis (CADe/CADx) category (5; 3.7%) focused on the real-time detection of lesions, especially in colorectal and gastric cancer, utilizing endoscopic and histopathological imaging. Finally, Generative AI (GenAI) (2; 1.5%), such as Midjourney and GPT-4-based image generators, was explored in the context of cervical cancer and dermatological manifestations of oncology treatments, particularly for educational or preventive applications. These associations highlight that ML/DL-based tools dominate the AI landscape in cancer research, while LLMs and domain-specific systems such as Watson are gaining space in clinical communication and decision-making, particularly in resource-limited settings (Table 221-28).
Table 2. Types and Models of Artificial Intelligence Employed
|
Category |
Description |
Count |
Percentage |
|
ML/DL |
ML/DL are subfields of AI that enable computer systems to automatically learn patterns and representations from data, improving performance on complex tasks without explicit programming21,22 |
96 |
73.9% |
|
LLMs / NLP-based |
LLMs and (NLP)-based systems are advanced AI techniques designed to understand, generate, and manipulate human language by leveraging vast datasets and deep neural network architectures23,24 |
19 |
14.2% |
|
GenAI |
GenAI refers to a class of AI models capable of creating new content, such as text, images, or data, by learning patterns from existing datasets and producing outputs that resemble human-generated information25 |
2 |
1.5% |
|
Watson for Oncology (IBM Watson) |
IBM Watson is an AI-powered clinical decision support system developed by IBM, designed to assist oncologists by analyzing large volumes of medical data and evidence-based guidelines to recommend personalized cancer treatment options26,27 |
5 |
3.7% |
|
CADe/CADx |
CADe and CADx refer to AI-driven systems that assist radiologists and clinicians by automatically identifying and characterizing abnormalities in medical images, thereby enhancing diagnostic accuracy and supporting clinical decision-making28 |
5 |
3.7% |
|
Others/Not clearly defined |
|
7 |
5.2% |
DISCUSSION
General Information
The sharp rise in oncology-focused AI publications beginning in 2022 can be attributed, in part, to the transformative impact of generative language models, particularly ChatGPT, on healthcare and related fields. Introduced by OpenAI in November 2022 using the GPT-3.5 architecture and followed by the GPT-4 release in March 2023, ChatGPT quickly demonstrated remarkable capabilities in generating human-like responses, understanding nuanced contexts, and supporting diverse applications in clinical communication, education, and patient engagement29. While ChatGPT alone does not account for the full surge in scientific output, as the current bibliometric findings reveal a wide variety of AI technologies applied in oncology, its influence has undeniably fueled academic and clinical interest. In January 2024, Traffic Analytics an advanced web traffic measurement tool developed by Semrush30, a global leader in online visibility data, reported 2.4 billion global visits to ChatGPT, a staggering 178.1% increase compared to the same period in 2023. Of these, 124 million interactions originated from Brazil, underscoring the global scale of adoption.
The United States and China emerged as the most prominent countries in terms of research output on AI applications in oncology. However, China’s absence from Figure supplementary 1 which illustrates countries with the highest ChatGPT-related activity suggests that Chinese contributions to AI in cancer care extend far beyond the implementation of generative language models. Indeed, the present review identified a variety of Chinese studies leveraging different AI technologies across multiple oncological domains. For example, Liu et al.31 reported the successful use of an AI-assisted home enteral nutrition (HEN) system to improve long-term outcomes in patients with stage III-IV nasopharyngeal carcinoma, demonstrating the integration of AI in supportive cancer care through intelligent monitoring and personalized nutrition management. Similarly, Yli-Hietanen et al.32 emphasized the strategic use of big data and intelligent modeling in Chinese oncology research, noting the critical role of biologically informed ML in improving predictive accuracy and clinical utility. This broad technological exploration highlights the need for bibliometric analyses that go beyond specific AI tools to fully capture thematic and methodological trends in global oncology research.
To ensure analytical clarity and methodological transparency, the Discussion was deliberately structured around two complementary pillars. The first pillar is grounded in the bibliometric results, directly anchored in the quantitative and descriptive findings of the analysis, including temporal publication trends, leading countries, volume of scientific output, types of artificial intelligence employed, and oncological domains addressed. This evidence-based pillar is primarily reflected in the sections General Information, Type of Artificial Intelligence Employed, and Artificial Intelligence in Cancer Control for Public Health Policies in Developing or Underdeveloped Countries, insofar as these sections interpret patterns, distributions, and gaps emerging from the bibliometric data. The second pillar encompasses analytical interpretation and technological projection, drawing on critical synthesis of the literature to contextualize the bibliometric findings and explore their implications for practice and policy. This interpretative pillar is represented in the sections Artificial Intelligence as a Solution in Cancer Control, Barriers to Artificial Intelligence in Cancer Control, and Implications for Public Policies and Brazil’s National Health System (SUS), which extend beyond bibliometric metrics to discuss conceptual, ethical, infrastructural, and governance-related dimensions of AI in oncology.
Artificial Intelligence as a Solution in Cancer Control
AI has emerged as a transformative force in the field of oncology, offering innovative solutions across diagnostic, therapeutic, and prognostic domains. Bongurala et al.33 emphasize that AI's integration into oncology is revolutionizing treatment decision-making by enabling precision medicine and enhancing efficiency in clinical workflows, especially in complex cases involving tumor genomics and molecular heterogeneity. Similarly, Butt et al.34 highlight that AI-driven systems significantly improve diagnostic accuracy and staging in endometrial cancer by automating histopathological interpretations and enhancing visual feature extraction from MRI images, thus enabling more targeted treatment interventions. These findings are reinforced by Aziz et al.35, who note that AI's ability to handle multimodal datasets facilitates timely cancer detection and stratification, particularly when combined with big data analytics and omics integration.
The versatility of AI is further demonstrated in the studies by Bongurala et al.33, where pediatric oncology also benefits from AI-enabled risk stratification and optimized therapy, contributing to improved survival rates and cost-effectiveness. Chen et al.36 also underscore AI's potential in clinical support, citing its role in reducing observer variability in radiology and pathology, which remains a cornerstone of early cancer diagnosis and monitoring. Furthermore, Bongurala et al.33 argue that future developments such as explainable AI and quantum computing will propel oncology into a new era of data-driven insights, with enhanced transparency and clinical applicability. The growing relevance of AI in therapeutic planning is supported by Kinikoglu and Isik37, who discuss the use of transformer-based models like ChatGPT in triage, education, and communication with cancer patients, particularly in resource-limited settings.
Importantly, these technological advances align with the strategic goals of public health systems, especially in middle-income countries like Brazil. Butt et al.34 demonstrate how AI can reduce unnecessary procedures and improve guideline adherence, a critical need in cost-sensitive healthcare environments. As Bongurala et al.33 articulate, AI-powered systems are uniquely positioned to support real-time decision-making, enhance personalized treatment regimens, and streamline oncology services, especially when integrated with national data infrastructures and digital registries. In this way, AI is not merely an auxiliary tool but a central pillar in the evolution of cancer control, particularly when supported by policies that ensure ethical implementation, robust data governance, and equitable access.
Barriers to Artificial Intelligence in Cancer Control
A significant barrier to the clinical integration of an AI in oncology lies in the limited generalizability of many models, which are often developed using homogenous datasets. Studies have shown that when these models are applied to diverse populations, their performance may degrade substantially due to a lack of consideration for local clinical practices, genetic variability, and environmental factors33,35. This issue is further compounded by the common absence of external validation datasets, which compromises the robustness and reproducibility of AI findings across different clinical settings. The risk of overfitting, where algorithms become excessively tailored to training data and fail to adapt to new inputs, remains a critical challenge, particularly in DL applications that involve vast parameter spaces and complex decision architectures36.
Another limitation centers on the dependency of AI systems on large, structured datasets, which are often fragmented, proprietary, or subject to regulatory constraints. As Chen et al.36 highlight, the lack of integrated and shareable data infrastructures inhibits the scalability of AI tools in oncology. Moreover, many high-performing models, especially those employing DP, are perceived as “black boxes,” offering little to no insight into the logic behind their outputs. This lack of transparency can erode clinician trust, hinder shared decision-making, and raise ethical concerns regarding algorithmic accountability. The issue becomes even more pronounced in generative models as ChatGPT, which have been observed to produce medically inaccurate or fictitious responses without referencing reliable sources, thereby introducing risks in clinical interpretation37-39.
Contextual and infrastructural mismatches further limit the applicability of AI tools across different healthcare systems. For instance, Liu et al.40 demonstrate how IBM Watson failed to align with Chinese clinical protocols, largely due to the exclusion of regionally common therapies and physiological nuances of the local population. Such discrepancies underline the importance of cultural and regional adaptability in AI model development. Additionally, the unequal distribution of healthcare resources poses another barrier, as low-income settings may lack the technological infrastructure or trained personnel required to implement AI-driven recommendations40,41. These challenges are exacerbated by the absence of clear regulatory guidelines and legal frameworks to govern the use of AI in oncology, leaving unresolved questions around liability and data security33,34. Addressing these multifaceted limitations is essential to ensure the safe, ethical, and equitable deployment of AI technologies in cancer care.
Cost-Effectiveness
Economic analyses show that AI can generate substantial cost savings in cancer control, with applications ranging from screening to digital health communication. Hassan et al.42 reported that the use of the GI GENIUS AI system in colonoscopy screenings for colorectal cancer in Italy resulted in a net saving of €14.34 per patient, primarily driven by a reduction in colorectal cancer (CRC) treatment costs (–€28.37) despite a marginal increase in screening (€10.50) and adenoma management (€3.53) expenses. Similarly, Areia et al.43 found that AI-assisted colonoscopy reduced per-person screening costs from $3400 to $3343 (a saving of $57), with a projected annual national savings of $290 million in the United States, while preventing 7194 CRC cases and 2089 deaths each year. In the domain of cervical cancer screening in China, Shen et al.44 demonstrated that AI-assisted liquid-based cytology (LBC) could achieve an incremental cost-effectiveness ratio (ICER) as low as $622 per QALY gained compared to no screening, with the most cost-effective strategy reaching $8790/QALY gained under certain cost conditions.
In prostate cancer diagnostics, Du et al.45 illustrated that an AI-assisted pathology workflow could reduce healthcare costs by 1.2% at an AI implementation cost of €10 per case, although higher AI operational costs (€100–€200 per case) rendered the human pathologist workflow dominant with ICER values exceeding €1 million per QALY gained. This emphasizes the sensitivity of cost-effectiveness to AI unit costs. Additionally, in a digital health communication context, Winterstein et al.46 evaluated an AI-generated social media influencer campaign for cancer prevention, achieving an average reach cost of only €0.013 per user, with the most cost-efficient strategy costing €0.006 per reach.
Aspects Related to Big Data
In the current landscape of oncology, the integration of Big Data has emerged as a transformative force, enabling the processing and interpretation of massive datasets to inform clinical decisions with greater precision and depth. According to Charalambous and Dodlek47, Big Data technologies allow clinicians and researchers to extract insights from vast, heterogeneous sources ranging from electronic health records (EHRs) to genomics and radiological images enabling advancements in diagnosis, prognostication, and personalized treatment pathways. This analytical power not only enhances early detection and risk stratification, but also enables real-time monitoring and adaptive management across the cancer care continuum. As highlighted by Nguyen, Tran, and Le48, such capabilities are especially vital in contexts like gastric cancer, where traditional drug discovery methods are costly and time-intensive. Big Data, when coupled with AI, allows for high-throughput analyses that accelerate the identification of therapeutic targets and prediction of compound efficacy and toxicity.
Moreover, Big Data analytics in oncology is instrumental in optimizing health system operations, resource allocation, and patient-centered care delivery. Charalambous and Dodlek47 emphasize the strategic role of Big Data in health behavior interventions, pharmacovigilance, and outcome estimations, thereby contributing to more sustainable healthcare systems. When integrated with advanced computing and DL techniques, these data-driven frameworks support the development of robust diagnostic models for conditions like lung cancer48. Altogether, the literature47-51 reflects that Big Data is not merely a technological asset, but a foundational element in the shift toward precision oncology, informing every stage from molecular research to bedside clinical decisions.
Implications for Public Policies and Brazil’s National Health System (SUS)
In the context of public policymaking, the rapid expansion of AI in oncology has reinforced the need to translate technological advances into actionable governance frameworks that can strengthen cancer control strategies within universal health systems. Evidence on early detection, risk stratification, treatment guidance, and health system optimization indicates that AI may accelerate clinical pathways and improve decision-making efficiency when aligned with regulatory safeguards and implementation readiness1-5. From a systems perspective, these advances imply that ministries of health and public institutions must develop policies that simultaneously foster innovation and ensure safety, transparency, and accountability, particularly when AI tools are integrated into screening programs, diagnostic workflows, and treatment planning supported by large-scale clinical and imaging datasets6-10.
However, policy translation remains constrained by persistent gaps in external validation, equity considerations, and real-world integration, which are critical for adoption in the Brazilian National Health System (SUS) and other resource-constrained settings. Studies11-13 highlight that many AI models remain proof-of-concept, and when implemented without robust validation across heterogeneous populations, they may amplify clinical uncertainty and exacerbate disparities in access and outcomes. In parallel14,15, ethical and regulatory challenges, such as data privacy, accountability, and the risk of bias, demand policy instruments that operationalize responsible AI governance, particularly in contexts where datasets may be fragmented and infrastructural capacity is uneven. For LMICs, the literature emphasizes that policy relevance depends on contextual adaptation, workforce training, and investments in digital infrastructure capable of supporting interoperable data ecosystems and equitable deployment, thereby enabling AI to function as a public health asset rather than an additional source of inequity in cancer control16-18.
Type of Artificial Intelligence Employed
AI in oncology has diversified into a rich ecosystem of technologies, each bringing specific capabilities to clinical practice. The analyzed articles present a range of AI types including traditional ML, DL, convolutional neural networks (CNNs), LLMs such as ChatGPT, and explainable AI (XAI). These AI types have been applied across the cancer care continuum from prevention to treatment demonstrating unique strengths. For instance, Suhail et al.52 describe the use of DL and ML to enhance early detection and prognosis prediction in hepatocellular carcinoma (HCC), integrating molecular signatures and radiomic data to guide personalized therapies. Similarly, the AI systems examined by Souadka et al.18 have enhanced image interpretation and intraoperative decision-making processes in surgical oncology, demonstrating particular relevance and applicability in low- and middle-income countries.
Beyond these examples, other AI modalities such as GenAI, vision transformers, and reinforcement learning are gaining traction in oncology. As highlighted by Wang et al.53, GenAI particularly in the form of multimodal models is revolutionizing cancer prevention by enabling communication-enhanced interventions, especially through intelligent agents and virtual companions. Meanwhile, the work of Patel et al.54 emphasizes the synergistic potential of combining AI and natural compounds in HCC management, showing that AI can optimize compound screening and treatment personalization. These findings reinforce that AI is not monolithic; its different variants yield complementary advantages, such as interpretability, speed, precision, and adaptability. Collectively, these diverse forms of AI justify their increasing deployment in oncology and substantiate the value of bibliometric reviews to map the technological landscape and inform strategic integration into clinical research and practice.
Study limitations
The absence of qualitative content analysis and the reliance on self-reported data from the articles hinder the precise identification of publication biases and the assessment of the actual maturity level of the AI technologies described for cancer control.
CONCLUSION
This bibliometric review offers a comprehensive and data-driven overview of AI applications in cancer control, highlighting both rapid technological advances and the heterogeneity of implementation and validation. The findings show a global trend positioning AI as a transformative tool for early detection, diagnostic precision, personalized treatment, and health system efficiency. Yet, significant challenges persist, including ethical concerns, infrastructural gaps, data governance issues, and limited external validation across diverse populations. Although high-income countries lead scientific output, growing contributions from low- and middle-income countries demonstrate rising interest in leveraging AI to reduce cancer control disparities. The scarcity of real-world clinical applications and cost-effectiveness analyses underscores the need for translational research that connects theoretical potential to practical use. Overall, the recent surge in publications reflects a shift toward responsible, equitable, and context-aware integration of AI in oncology, with important implications for clinical practice and public health policy.
ACKNOWLEDGEMENT
The authors thank Manuella Salm Coelho and Robson Moraes da Silva for their guidance with the creation of the images.
CONTRIBUTIONS
All the authors contributed to the process of preparation, writing, data collection and analysis, review and editing of the manuscript. They approved the final version for publication.
DECLARATION OF CONFLICT OF INTERESTS
The author Carina Munhoz de Lima declares a potential conflict of interest due to being part of the editorial team of INCA’s Revista Brasileira de Cancerologia. The other authors do not have any conflict of interest.
DATA AVAILABILITY STATEMENT
All the contents associated with the article are included in the manuscript.
FUNDING SOURCES
None.
REFERENCES
1. Jones OT, Matin RN, van der Schaar M, et al. Artificial intelligence and machine learning algorithms for early detection of skin cancer in community and primary care settings: a systematic review. Lancet Digit Health. 2022;4(6):e466-76. doi: https://www.doi.org/10.1016/S2589-7500(22)00023-1
2. Jiang Y, Wang C, Zhou S. Artificial intelligence-based risk stratification, accurate diagnosis and treatment prediction in gynecologic oncology. Semin Cancer Biol. 2023;96:82-99. doi: https://www.doi.org/10.1016/j.semcancer.2023.09.005
3. Mitsala A, Tsalikidis C, Pitiakoudis M, et al. Artificial intelligence in colorectal cancer screening, diagnosis and treatment: a new era. Curr Oncol. 2021;28(3):1581-607. doi: https://www.doi.org/10.3390/curroncol28030149
4. Uwimana A, Gnecco G, Riccaboni M. Artificial intelligence for breast cancer detection and its health technology assessment: a scoping review. Comput Biol Med. 2025;184:109391. doi: https://www.doi.org/10.1016/j.compbiomed.2024.109391
5. Cortlana VM, Itodo K, Leyfman Y, et al. Artificial intelligence in cancer care: addressing challenges and health equity. Oncology. 2025;39(3):105-10. doi: https://www.doi.org/10.46883/2025.25921037
6. Avanzo M, Wei L, Stancanello J, et al. Machine and deep learning methods for radiomics. Med Phys. 2020;47(5):e185-202. doi: https://www.doi.org/10.1002/mp.13678
7. Issa NT, Stathias V, Schürer S, et al. Machine and deep learning approaches for cancer drug repurposing. Semin Cancer Biol. 2021;68:132-42. doi: https://www.doi.org/10.1016/j.semcancer.2019.12.011
8. Sultan AS, Elgharib MA, Tavares T, et al. The use of artificial intelligence, machine learning and deep learning in oncologic histopathology. J Oral Pathol Med. 2020;49(9):849-56. doi: https://www.doi.org/10.1111/jop.13042
9. Tran KA, Kondrashova O, Bradley A, et al. Deep learning in cancer diagnosis, prognosis and treatment selection. Genome Med. 2021;13(1):152. doi: https://www.doi.org/10.1186/s13073-021-00968-x
10. Liu Y, Ji Y, Chen J, et al. Pioneering noninvasive colorectal cancer detection with an AI-enhanced breath volatilomics platform. Theranostics. 2024;14(11):4240-55. doi: https://www.doi.org/10.7150/thno.94950
11. Lami K, Yoon HS, Parwani AV, et al. Validation of prostate and breast cancer detection artificial intelligence algorithms for accurate histopathological diagnosis and grading: a retrospective study with a Japanese cohort. Pathology. 2024;56(5):633-42. doi: https://www.doi.org/10.1016/j.pathol.2024.02.009
12. Lyman GH, Kuderer NM. Artificial intelligence in cancer clinical research: II. development and validation of clinical prediction models. Cancer Invest. 2024;42(6):447-51. doi: https://www.doi.org/10.1080/07357907.2024.2354991
13. Raciti P, Sue J, Retamero JA, et al. Clinical validation of artificial intelligence–augmented pathology diagnosis demonstrates significant gains in diagnostic accuracy in prostate cancer detection. Arch Pathol Lab Med. 2023;147(10):1178-85. doi: https://www.doi.org/10.5858/arpa.2023-0143-OA
14. Gordon ER, Trager MH, Kontos D, et al. Ethical considerations for artificial intelligence in dermatology: a scoping review. Br J Dermatol. 2024;190(6):789-97. doi: https://www.doi.org/10.1111/bjd.22123
15. Shah SFH, Arecco D, Draper H, et al. Ethical implications of artificial intelligence in skin cancer diagnostics: use-case analyses. Br J Dermatol. 2025;192(3):520-9. doi: https://www.doi.org/10.1093/bjd/ljae434
16. Banatwala U, Ibrahim MT, Shaikh RH, et al. A comprehensive exploration of artificial intelligence in orthopaedics within lower-middle-income countries: a narrative review. J Pak Med Assoc. 2024;74(Suppl 4):S90-6. doi: https://www.doi.org/10.47391/JPMA.AKU-9S-14
17. Mollura DJ, Culp MP, Pollack E, et al. Artificial intelligence in low- and middle-income countries: innovating global health radiology. Radiology. 2020;297(3):513-20. doi: https://www.doi.org/10.1148/radiol.2020201434
18. Souadka A. Artificial intelligence in surgical oncology: enhancing precision and personalized treatment in low- and middle-income countries. J Surg Oncol. 2024;130(2):341-2. doi: https://www.doi.org/10.1002/jso.27733
19. Donthu N, Kumar S, Mukherjee D, et al. How to conduct a bibliometric analysis: an overview and guidelines. J Bus Res. 2021;133:285-96. doi: https://www.doi.org/10.1016/j.jbusres.2021.04.070
20. Page MJ, Moher D, Bossuyt PM, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021;372:n160. doi: https://www.doi.org/10.1136/bmj.n160
21. Jiao Z, Hu P, Xu H, et al. Machine learning and deep learning in chemical health and safety: a systematic review of techniques and applications. J Chem Health Saf. 2020;27(6):316-34. doi: https://www.doi.org/10.1021/acs.chas.0c00075
22. Kumar K, Chaudhury K, Tripathi SL. Future of machine learning and deep learning in healthcare monitoring system. In: Ghai D, Tripathi SL, Saxena S, et al. Machine learning algorithms for signal and image processing. Nova Jersey: Wiley; 2022. doi: https://www.doi.org/10.1002/9781119861850.ch17
23. Venkatasubramanian V, Chakraborty A. Quo vadis ChatGPT? From large language models to large knowledge models. Comput Chem Eng. 2025;192:108895. doi: https://doi.org/10.1016/j.compchemeng.2024.108895
24. Pais S, Cordeiro J, Jamil MLJ. NLP-based platform as a service: a brief review. J Biomed Data. 2022;9(1):54. doi: https://doi.org/10.1186/s40537-022-00603-5
25. Ghimire P, Kim K, Acharya M. Generative AI in the construction industry: opportunities and challenges. arXiv [preprint]. 2023. doi: https://doi.org/10.48550/arXiv.2310.04427
26. Zhou N, Zhang CT, Lv HY, et al. Concordance study between IBM Watson for oncology and clinical practice for patients with cancer in China. Oncologist. 2019;24(6):812-9. doi: https://doi.org/10.1634/theoncologist.2018-0255
27. Park T, Gu P, Kim C-H, et al. Artificial intelligence in urologic oncology: the actual clinical practice results of IBM Watson for Oncology in South Korea. Prostate Int. 2023;11(4):218-21. doi: https://doi.org/10.1016/j.prnil.2023.09.001
28. Dhull A, Gupta G. An intelligent two phase fuzzy decision tree based clustering model for design of computer aided detection/diagnosis (CADe/CADx) system. J Med Syst. 2018;33(1):63-75. doi: https://doi.org/10.1007/s12647-017-0230-8
29. Khan N, Kumar S, Mukherjee D, et al. Global insights and the impact of generative AI–ChatGPT on multidisciplinary: a systematic review and bibliometric analysis. Cognit Syst Res. 2024;36(1):2353630. doi: https://doi.org/10.1080/09540091.2024.2353630
30. Kelly B. Investigating ChatGPT search: insights from 80 million clickstream records [Internet]. Boston: Semrush; 2025 [cited 2025 Sep 29]. Available from: https://www.semrush.com/blog/chatgpt-search-insights/
31. Liu J, Wang X, Ye X, et al. Improved health outcomes of nasopharyngeal carcinoma patients 3 years after treatment by the AI-assisted home enteral nutrition management. Front Nutr. 2025;11:1481073. doi: https://doi.org/10.3389/fnut.2024.1481073
32. Yli-Hietanen J, Ylipää A, Yli-Harja O. Cancer research in the era of next-generation sequencing and big data calls for intelligent modeling. Chin J Cancer. 2015;34(10):423-6. doi: https://doi.org/10.1186/s40880-015-0008-8
33. Bongurala AR, Save D, Virmani A. Progressive role of artificial intelligence in treatment decision-making in the field of medical oncology. Front Med. 2025;12:1533910. doi: https://doi.org/10.3389/fmed.2025.1533910
34. Butt SR, Soulat A, Lal PM, et al. Impact of artificial intelligence on the diagnosis, treatment and prognosis of endometrial cancer. Ann Med Surg (Lond). 2024;86(3):1531-9. doi: https://doi.org/10.1097/MS9.0000000000001733
35. Aziz M, Ejaz SA, Zargar S, et al. Deep learning and structure-based virtual screening for drug discovery against NEK7: a novel target for the treatment of cancer. Molecules. 2022;27(13):4098. doi: https://doi.org/10.3390/molecules27134098
36. Chen ZH, Lin L, Wu CF, et al. Artificial intelligence for assisting cancer diagnosis and treatment in the era of precision medicine. Cancer Commun (Lond). 2021;41(11):1100-15. doi: https://doi.org/10.1002/cac2.12215
37. Kinikoglu O, Isik D. Evaluating the performance of ChatGPT-4 o oncology expert in comparison to standard medical oncology knowledge: a focus on treatment-related clinical questions. Cureus. 2025;17(1):e78076. doi: https://doi.org/10.7759/cureus.78076
38. Alsayed AA, Aldajani MB, Aljohani MH, et al. Assessing the quality of AI information from ChatGPT regarding oral surgery, preventive dentistry, and oral cancer: an exploration study. Saudi Dent J. 2024;36(11):1483-9. doi: https://doi.org/10.1016/j.sdentj.2024.09.009
39. Ebner F, Hartkopf A, Veselinovic K, et al. A comparison of ChatGPT and multidisciplinary team meeting treatment recommendations in 10 consecutive cervical cancer patients. Cureus. 2024;16(8):e67458. doi: https://doi.org/10.7759/cureus.67458
40. Liu C, Liu X, Wu F, et al. Using artificial intelligence (Watson for Oncology) for treatment recommendations amongst Chinese patients with lung cancer: feasibility study. J Med Internet Res. 2018;20(9):e11087. doi: https://doi.org/10.2196/11087
41. Kim M, Park H, Kho B. Artificial intelligence and lung cancer treatment decision: agreement with recommendation of multidisciplinary tumor board. Transl Lung Cancer Res. 2020;9(3):507-14. doi: https://doi.org/10.21037/tlcr.2020.04.11
42. Hassan C, Povero M, Pradelli L, et al. Cost-utility analysis of real-time artificial intelligence-assisted colonoscopy in Italy. Endosc Int Open. 2023;11(11):E1046-55. doi: https://doi.org/10.1055/a-2136-3428
43. Areia M, Mori Y, Correale L, et al. Cost-effectiveness of artificial intelligence for screening colonoscopy: a modelling study. Lancet Digit Health. 2022;4(6):e436-44. doi: https://doi.org/10.1016/S2589-7500(22)00042-5
44. Shen M, Zou Z, Bao H, et al. Cost-effectiveness of artificial intelligence-assisted liquid-based cytology testing for cervical cancer screening in China. Lancet Reg Health West Pac. 2023;34:100726. doi: https://doi.org/10.1016/j.lanwpc.2023.100726
45. Du X, Hao S, Olsson H, et al. Effectiveness and cost-effectiveness of artificial intelligence–assisted pathology for prostate cancer diagnosis in Sweden: a microsimulation study. Eur Urol Oncol. 2025;8(1):80-6. doi: https://doi.org/10.1016/j.euo.2024.05.004
46. Winterstein JT, Abels J, Kuehn A, et al. AI-generated cancer prevention influencers can target risk groups on social media at low cost. Eur J Cancer. 2025;217:115251. doi: https://doi.org/10.1016/j.ejca.2025.115251
47. Charalambous A, Dodlek N. Big data, machine learning, and artificial intelligence to advance cancer care: opportunities and challenges. Semin Oncol Nurs. 2023;39(3):151429. doi: https://doi.org/10.1016/j.soncn.2023.151429
48. Nguyen MH, Tran ND, Le NQK. Big data and artificial intelligence in drug discovery for gastric cancer: current applications and future perspectives. Curr Med Chem. 2025;32(10):1968-86. doi: https://doi.org/10.2174/0929867331666230913105829
49. Guan P, Yu K, Wei W, et al. Big data analytics on lung cancer diagnosis framework with deep learning. Trans Comput Biol Bioinform. 2024;21(4):757-68. doi: https://doi.org/10.1109/TCBB.2023.3281638
50. Wei L, Huang Y, Chen Z, et al. Artificial intelligence combined with big data to predict lymph node involvement in prostate cancer: a population-based study. Front Oncol. 2021;11:763381. doi: https://doi.org/10.3389/fonc.2021.763381
51. Dlamini Z, Francies FZ, Hull R, et al. Artificial intelligence and big data in cancer and precision oncology. Comput Struct Biotechnol J. 2020;18:2300-11. doi: https://doi.org/10.1016/j.csbj.2020.08.019
52. Suhail M, Tarique M, Tabrez S, et al. Leveraging AI and natural compounds: innovative approaches in the diagnosis and treatment of hepatocellular carcinoma. Curr Pharm Des. 2025;31:1-11. doi: https://doi.org/10.2174/0113816128364693250117060342
53. Wang Y, Lin W, Zhuang X, et al. Advances in artificial intelligence for the diagnosis and treatment of ovarian cancer. Oncol Rep. 2024;51(3):46. doi: https://doi.org/10.3892/or.2024.8705
54. Patel R, Jain A, Patel Z, et al. Artificial intelligence and machine learning in hepatocellular carcinoma screening, diagnosis and treatment: a comprehensive systematic review. Glob Acad J Med Sci. 2024;6(2):83-97. doi: https://doi.org/10.36348/gajms.2024.v06i02.007
Recebido em 2/12/2025
Aprovado em 26/1/2026
Scientific-editor: Anke Bergmann. Orcid iD: https://orcid.org/0000-0002-1972-8777
![]()
Este é um artigo publicado em acesso aberto (Open Access) sob a licença Creative Commons Attribution, que permite uso, distribuição e reprodução em qualquer meio, sem restrições, desde que o trabalho original seja corretamente citado.